Table of Contents
New Zealand Doctors Speaking Out with Science
New Zealanders have been praised as efficient “lockdowners” by those who consider lockdown to be a public health intervention with merit. Whilst our counterparts in places such as the UK and parts of the USA faced strict lockdown measures concurrent with high transmission and mortality rates, New Zealand appeared to fare well simply by following similar, if not the same, measures.
How could this have happened if not for “efficient lockdown”? This is a classic case of post hoc ergo propter hoc fallacy: Y followed X, therefore Y was caused by X. In epidemiology this is known as confirmation bias, whereby “expected relationships are confirmed, and unexpected relationships remain undiscovered, even when their unveiling would have important informational value.“
The idea that New Zealand’s low pre-vaccination covid-19 rates were due to lockdown is problematic for three main reasons. Firstly, nations along the Pacific Rim (specifically east and south-east Asia, and the south Pacific), with vastly different policy responses, many with multiple loosely-controlled land borders and without the facility to lockdown, fared similarly. British Pathologist and Hart Group member Dr John Lee offers the hypothesis that this may be due to exposures to other coronaviruses offering cross-immunity in a region where such viruses are most common, in this interesting and informative Unlocked interview (at 28m15s).
Secondly, airborne viruses survive and transmit in multiple and largely unidentified ways so that the elimination strategy enforced by governments using lockdown was always guaranteed to fail. Latent infections reactivated due to conditions in the immune system such as low Vitamin D, is one possible mechanism. This may have been the reason for a 1973 outbreak of probable coronavirus amongst Antarctic base workers who had remained in complete isolation for 17 weeks. It may also explain why populations across the world with limited and even absent Covid experienced a surge within weeks of the immune-suppressing “vaccine” rollout.
Anyone with experience in outbreak control will tell you that most investigations, even those with a central source such as contaminated food which is much easier to track and trace than viruses floating on air currents for hours to days, fail to identify the source and/or every infected contact. In fact, contact tracing for airborne viruses is considered futile except in specific situations.
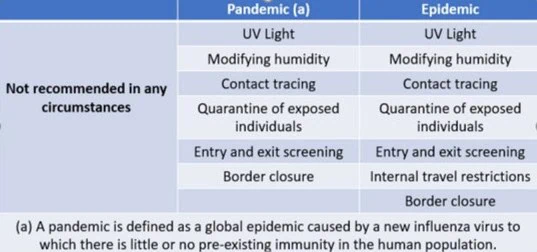
This was documented practice until covid, including DA Henderson et al’s 2006 key article Disease Mitigation Measures in the Control of Pandemic Influenza and the World Health Organization‘s systematic review of the evidence in 2019. On page 3 of the WHO document, Table 1: Recommendations on the use of non pharmaceutical interventions by severity level includes the following advice.
Thirdly, rather than stopping viral spread, lockdown shifted the burden of infection onto the most vulnerable (lower socio-economic; older; more co-morbidities), who were unable to maintain limited contact by working from home. It is reasonable to consider the possibility that New Zealand’s higher-risk population, who continued to have human contact during lockdown, had a baseline rate of cross-immunity.
On the other hand, our nursing home residents fared proportionally worse than non nursing home residents compared with other nations, at 64% of total deaths as at December 2021 compared with a weighted average of 30%. Could this be because of immune senescence (weakened immunity due to old age) in an otherwise immune population? We cannot know because antibody testing was not made available in New Zealand despite being accessible elsewhere. This seemed a strange policy during an epidemic threat, when prior exposure would have been useful information, especially for those working with our most vulnerable such as nursing home residents.
As far back as the Athenian plague in ~400BC, the disease-recovered were considered safe to care for the ill based on a recognition of natural immunity. Why was antibody testing unavailable to the New Zealand population?
It is apparent that lockdown in fact had no protective effect whatsoever. Public health officials have themselves confirmed that the purpose of lockdown was not to affect virus transmission, but to nudge the population towards accepting vaccination. This includes advisors as far removed from each other as Anthony Fauci in the USA, Matt Hancock in the UK and Michael Baker here in New Zealand. The conflicts of interest of Fauci and Hancock have come to light. We fully expect Baker’s conflicts to be revealed in due course.
Did Lockdown Harm New Zealanders?
We start by suggesting that “lockdown” is a term used in criminal incarceration which holds no place within health care terminology. It is now apparent that the use of language such as “go hard on the virus”, “let it rip”, “countermeasures” and “lockdown” encouraged acceptance of authoritarian policies employed against populations with military aggression. We share history scholar Naomi Wolf’s perspective in regard to the actual purposes of lockdown.
Privileged New Zealanders enjoyed lockdown. They tended to their gardens, walked their dogs, painted and renovated their homes, enjoyed time with their families. They joked about wanting another lockdown so that they could finish their home projects.
This was not the case for the many who suffered business closure, unemployment, an inability to pay their mortgage or rent, and struggled to feed their families. In a 2022 report Profiting from Pain, Oxfam described the surge in billionaire wealth simultaneous to the cost of living crisis experienced by millions worldwide, caused by the Covid-19 response. The world’s poorest suffered the most, which translates in each nation to the most vulnerable sections of society. Unelected billionaires benefiting from the response happen to be the same people pushing policies such as lockdown and mass vaccination onto humanity. An unprecedented and sinister conflict of interest.
The combination of 33 days at Level 4 lockdown (‘elimination’ level) and 19 days at Level 3 (‘restrict’ level) imposed by the New Zealand government between March and May of 2020 cost the economy at least 3.3% of GDP whilst resulting in little to no health benefit. Government documents show that these lockdown decisions were informed by mathematical modellers at Imperial College London and Otago University, acknowledged as alarmist and repeatedly wrong.
Socio-economic factors play a significant role across the lifespan, in determining population health outcomes. The health of our physical, social and economic environment, including education, employment and income opportunities, determines how healthy a population will be. This is even acknowledged by World Health Organization, although we now know that their focus has moved away from supporting a decentralised approach based on local context to achieve improved health outcomes, towards a focus on centralised control. An initial forewarning of this came as early as February 2020 when the world was told to copy China’s lockdown model.
It comes as no surprise then, that even without the catastrophic harms of the injectable Covid-19 products, the health of New Zealanders has suffered and will continue to suffer as a direct consequence of lockdown. Children appear to have suffered the worst due to lockdown policies. A pandemic of child abuse has been documented, resulting from forced isolation at home with abusers and reduced contact with the adults who offer protection, such as teachers. Whilst research on the health harms associated with lockdown specific to the New Zealand population is limited, an increase in delayed health care was experienced, particularly for vulnerable infants.
While harms of lockdowns are being well documented, the NZ Royal Commission of Inquiry is investigating the best ways (legislative, regulatory, and operational) to do this all again, but even better, when the next pandemic, or other emergency, miraculously appears.








{kind=link}