
Archaeological evidence suggests that tobacco was discovered in the Americas and was being cultivated and used by the indigenous culture as early as 5000 BC. It was introduced to Europe in the 16th century and became popular as smoking was often associated with a certain level of status or sophistication. In many cultures smoking was considered fashionable and associated with the upper classes or influential individuals – leading to the growth of the tobacco industry. New Zealand was no exception to this. The renowned New Zealand artist, Charles F Goldie, even depicted this devotion in his paintings of Maori women.
Smoking has continued to be popular among the Maori (and Pacific Islander) communities to this day, despite numerous campaigns to reduce or eradicate the habit. The communities and the individuals involved are aware of the dangers of smoking.
Intergenerational issues are problems or behaviours that persist through multiple generations within a family or society. If parents or family members smoke, it can increase the likelihood of children growing up in an environment where smoking is normalised or accepted. This exposure and influence may make children more likely to start smoking themselves. Various additional factors can be at play in intergenerational smoking. These may include shared genetic predispositions to addiction, social and cultural norms within the family, imitation of parental behaviour and exposure to smoking cues or environments.
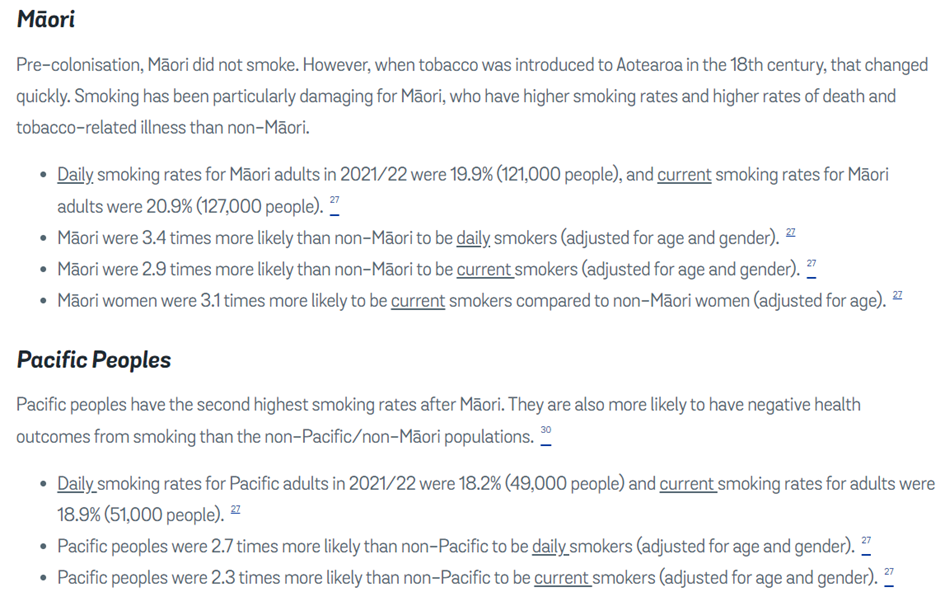
According to the World Health Organization (WHO), tobacco smoking is estimated to cause more than eight million deaths per year globally. This includes deaths from direct tobacco use and secondhand smoke exposure. It is likely that smoking can be held accountable for some of the disparate health outcomes between different populations. For example, from the smokefree.org.nz website we have the following information about frequency of smoking among different ethnic groups in NZ:
Authors Note: The smokefree.org.nz website has peddled misinformation. Before the introduction of tobacco to New Zealand, the Maori people had their own traditional smoking practices. They used a variety of native plants for smoking, including:
- Kawakawa (Macropiper excelsum): The leaves of the kawakawa plant were dried, rolled and smoked. Kawakawa was highly valued for its medicinal properties and was often used in traditional Maori herbal remedies.
- Manuka (Leptospermum scoparium): Manuka leaves were also dried and smoked. Manuka smoke was used for both medicinal and aromatic purposes.
- Pohutukawa (Metrosideros excelsa): The bark of the pohutukawa tree was sometimes used for smoking, primarily for its aromatic qualities.
Quitting smoking has been shown to have significant health benefits and can increase life expectancy. According to the US Centre for Disease Control and Prevention (CDC) ], smokers die an average of ten years earlier than nonsmokers.
Despite ample evidence of the harmful effects of smoking, Debbie Ngarewa-Packer (Co-Leader of Te Paati Maori) attributes the disparities in Maori and Pasifika health outcomes, such as lower life expectancy, solely to factors like “institutional racism” and “unconscious bias”. While I won’t address the issue of institutional racism, regarding unconscious bias Debbie might have a point. Unconscious bias refers to implicit attitudes, beliefs or stereotypes that individuals hold without conscious awareness. It is possible for individuals, including smokers, to develop unconscious biases towards cigarettes. Several factors can contribute to these biases. These may include:
- Conditioning: Over time, smokers develop associations between smoking and certain situations, emotions or activities. These associations can create an unconscious bias towards cigarettes, as the act of smoking becomes linked with pleasurable or comforting experiences.
- Social influences: Society and culture play a significant role in shaping individuals’ perceptions and biases. If a person is surrounded by friends, family members or peers who smoke or have positive attitudes towards smoking, it can influence their unconscious biases and perceptions of cigarettes.
- Addiction and dependence: Nicotine, the addictive substance in cigarettes, can alter brain chemistry and create a physiological dependency. This addiction can lead to unconscious biases as smokers may rationalise or justify their smoking behaviour to support their addiction.
- Marketing and advertising: Cigarette companies have historically employed marketing strategies to shape perceptions and create positive associations with their products. These strategies, which may include branding, imagery and lifestyle associations, can contribute to unconscious biases towards cigarettes among both smokers and non-smokers.
I suggest that Labour, Te Paati Maori and the upcoming government address the four noted issues when addressing the health disparities faced by Maori and Pasifika communities, instead of making health decisions based on race. It is challenging to accurately determine the extent to which personal or population addiction contributes to the disparities in health outcomes.
Non-smokers (and other groups) should not be penalised by one group’s inability to exercise self-control and personal sovereignty.






{kind=link}