
Table of Contents
Miguel’
While browsing the internet yesterday afternoon, I came across the following article in the NZ Herald:

The article reports on a recently published report from the Ministry of Health. Drawing on this report, the article states:
“While age was the single biggest determinant of risk of death – the bulk of Covid-19 mortalities to date have been recorded among Kiwis over 80 – vaccination status also mattered.
The analysis showed a 62 per cent reduction of risk of death among those who’d received two or more doses – and there was evidence, which future studies would explore further, that boosting lowered that danger even more.”
Curious, I followed the link to the MoH website:
On this summary page is another link to the report itself:
Click to access covid-19_mortality_in_aotearoa_inequities_in_risk_september_2022_29_sept.v2.pdf
After looking through the text, we get to the tabulated results on page 26.
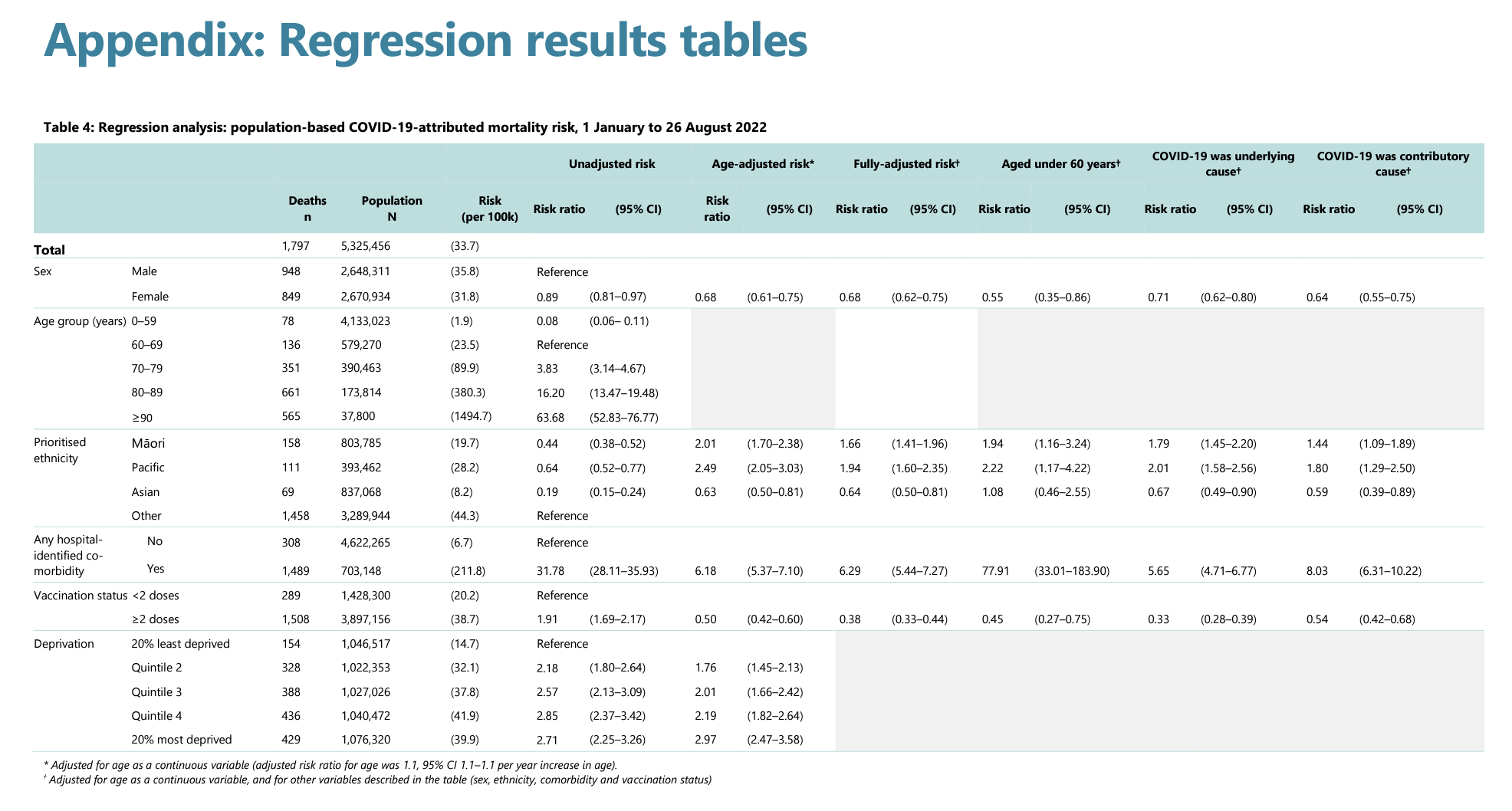
Sure enough, on the “vaccination status” row we can see a fully-adjusted risk of 0.38 for people with two or more doses of the vaccine, meaning they have only 38% of the risk of dying versus those with zero or only one dose (ie. Unvaccinated or partially-vaccinated).
But hang on a moment…
What’s this “fully-adjusted risk” business…?
Looking carefully, on the same row we see the “unadjusted risk.” In this column, which is essentially the raw data, those with 2+ doses of the vaccine have a risk-ratio of 1.91, meaning they are almost twice as likely to die as the unvaccinated and partially-vaccinated. (Remember that this is official MoH-published data.)
Reading the footnote on the table, we see that “fully-adjusted” is:
“Adjusted for age as a continuous variable, and for other variables described in the table (sex, ethnicity, comorbidity and vaccination status)”
That’s quite the list of adjustments. They’ve removed the effect of age – which they (and the NZ Herald article) acknowledge is a key influence – as well as the presence of significant comorbidities. But is this a reasonable adjustment?
Look at the unadjusted risk ratio for comorbidities: 31.78! Having a comorbidity, perhaps such as being obese or having heart disease, means you’re over 30x more likely to die from Covid-19 than not. Similarly, when you look at age groups: being in your 80s means your risk is some 16x higher of dying from Covid-19 than someone in their 60s.
Is it a reasonable adjustment, then, to statistically separate two of the most material risks from the analysis to report an ‘adjusted’ benefit of 2+ doses of the Covid-19 vaccine? After all, removing these factors turns an ~2x increased risk of dying from Covid-19 (having had 2+ vaccine doses) into a ~2/3 decreased risk.
I could accept the argument that the unvaccinated are (I’m guessing here) a younger cohort than the double-dosed, and the older you are, the more likely you are to die, so they want to even the playing field. In a purely academic sense, sure, but if this analysis is used to support public policy (such as mandates and vaccine passes) I would argue that age is best analysed after vaccination status. That is, show us the data of deaths by age-group, adjusted for vaccination status. Do older people who have had 2+ doses fare better than those who have not? After all, the vaccines are something individuals (and the government) can influence, but age is not. You are the age you are, and so – I would argue – removing the (major) influence of age to present a case for vaccine efficacy renders the conclusion redundant.
Let’s step back for a moment, too. Remember “95% effective”…? I sure do. How the Dickens, then, does such a “safe and effective” vaccine show (in unadjusted data) an increased risk of dying versus those who’ve had none? Surely, even not removing the (large) influence of age and comorbidities, we should see the, well, efficacy of the safe-and-effective vaccine in the raw numbers. And we’re not talking about a small difference here – nearly twice as many people per 100,000 cases died fully-vaccinated versus un- and partially-vaccinated. Effective…? The vaccine only shows efficacy when two major factors are removed.
And why are the partially vaccinated grouped in with the unvaccinated?
I would argue that those who’ve had one dose only are closer in effect to the 2+ dose cohort than they are to the unvaccinated. Surely some medicine is better than none, right? Why blur the lines by lumping them together? I have seen the argument elsewhere that the partially vaccinated are such a small cohort that they are not reasonably analysed on their own. This is fair enough, but I would suggest they’re best placed in the ‘vaccinated’ bucket. It would be interesting to know how this affected the results, which brings me to another point.
Disappointingly, the raw data used in this report is not shared, nor are the models/equations that resulted from this analysis. Those of us outside the MoH do not have the same opportunity to reproduce this data, or test different combinations or approaches. Also absent is any authorship or contact information; there is no ability to ask questions of the team who assembled the report.
I’m sure there is more to this report than my weak review has presented here, but one closing observation. For the period analysed – 1 January 2022 to 26 August 2022 – 33.7 people died out of every 100,000 who tested positive for Covid-19. This means that having tested positive, there was on average a 1-in-3000 chance of dying. One in three thousand? Did this disease justify the response?








{kind=link}