
Table of Contents
Cranmer
Lawyer with over 25 years experience in some of the world’s biggest law firms. I divide my time between the UK and NZ. This Substack explores issues facing NZ at present under my nom du plume, Cranmer.
As part of New Zealand’s provisional approval of the Pfizer vaccine, the country’s regulator Medsafe prepared a Non-Clinical Assessment in January 2021 which concluded that:
- the lipid nanoparticles were distributed through the body, mainly into the liver, adrenal glands, spleen and ovaries.
- with regard to pregnancy, “although not directly addressable from the nonclinical data, there may be a basis in the current circumstances for concluding the risk of vaccination during pregnancy is outweighed by the potential benefits of immunity particularly for specific subpopulations at heightened risk.”
- the proposed data sheet notes that there is limited experience in pregnant women and provides appropriately cautious advice that, “Administration of Comirnaty in pregnancy should only be considered when the potential benefits outweigh any potential risks for mother and fetus.”
Despite Medsafe’s assessment, the Medical Council issued guidance to all GPs in April 2021 which instructed doctors to only discuss the benefits of vaccination and warned that there “was no place for anti-vaccination messages in professional health practice, nor any promotion of anti-vaccination claims including on social media and advertising by health practitioners”.
The Medical Council has been unable to define what claims would be considered “anti-vaccination” and what advice would be considered appropriate and in accordance with the Medical Council’s existing guidance on informed consent which includes “highlighting risks specific to your patient”.
Medsafe’s Non-Clinical Assessment
Medsafe’s Non-Clinical Assessment was completed on 28 January 2021. The non-clinical assessment is a series of studies and evaluations that are conducted to assess the safety of a new drug or vaccine before it is tested in humans. Non-clinical assessments are usually conducted in animal models, and they provide important information about the pharmacological properties of the vaccine, its potential toxicity, and its effects on different organ systems.
Pfizer provided the identical nonclinical data to both Australia’s regulator, the TGA and New Zealand’s Medsafe. The interim TGA evaluation report was completed in early December 2020 and was provided to Medsafe who used it as the primary basis for its Non-Clinical Assessment. Studies evaluated by the TGA were not re-evaluated by Medsafe other than to verify the conclusions of the TGA against the submitted studies. Where the TGA had evaluated an interim report for a study that was subsequently updated with the final data, or where the study had been submitted to Medsafe after the TGA had finalized its interim report, that study was evaluated in detail by Medsafe and set out in its Non-Clinical Assessment.
When Medsafe was required, pursuant to an Official Information Act request in August 2021, to provide its approval documentation for the Pfizer vaccine, it provided 18 documents totalling 162 pages. In relation to its Non-Clinical Assessment, it only provided the first five pages of the 57 page document which only covered the table of contents and the first page of its introduction. Pages 6 to 57 were withheld in full.
The Lipid Nano-Particles (LNP)
LNPs are essentially very tiny bubbles of fat that are used to deliver genetic material into the cells. In the case of Pfizer’s vaccine, the payload is a messenger RNA molecule that encodes the spike protein from SARS-CoV-2.
The LNP component of the vaccine contains four lipids, two of which are described as “novel excipient lipids”. The Medsafe assessment notes that these two lipids are not listed on the TGA’s ingredient database and are therefore novel, both structurally and pharmaceutically. The report states that these lipids are a key aspect of the formulation contributing both to particle size of the LNPs and the stability of the mRNA in the formulation.
The report notes that because of the mechanism of action of most vaccines, pharmacokinetic studies are not normally a critical or significant aspect of a vaccine’s efficiency and/or safety assessment and not routinely required under relevant guidelines. However because “uptake of the LNP carrier” for the Pfizer vaccine is considered critical to its efficacy and because the vaccine contains two new excipients, pharmacokinetic studies were performed in this case.
These pharmacokinetic studies evaluate the absorption, distribution, metabolism, and elimination of the drug in animals (in the case of the Pfizer vaccine, the animals were mice, rats and nonhuman primates). This helps determine how the drug behaves in the human body and how much of the drug reaches the target site.
However, contrary to the repeated claims by the government throughout the pandemic that the vaccine remains largely in the arm before degrading, these studies clearly demonstrate that the lipids are distributed to the major organs of the body.
Within pharmacokinetics, biodistribution studies are used to determine how a drug or vaccine is distributed throughout the body after administration. This includes examining the concentrations of the substance in various organs, tissues, and fluids, as well as the mechanisms by which the substance is transported and eliminated from the body.
For the purpose of the biodistribution studies for its vaccine, Pfizer only measured the distribution of the lipids rather than the mRNA. This was an issue that was flagged by other national and supranational regulators during their assessments of the vaccine. The Medsafe assessment sets out questions that the Australian and European regulators asked Pfizer, together with Pfizer’s response and an observation from Medsafe.
In relation to the Pfizer biodistribution studies, the Australian TGA asked Pfizer why no tissues/organs were collected to analyse the distribution of the mRNA/expressed protein. Pfizer’s response was that the Spike protein distribution will mirror that of the lipid nanoparticles.
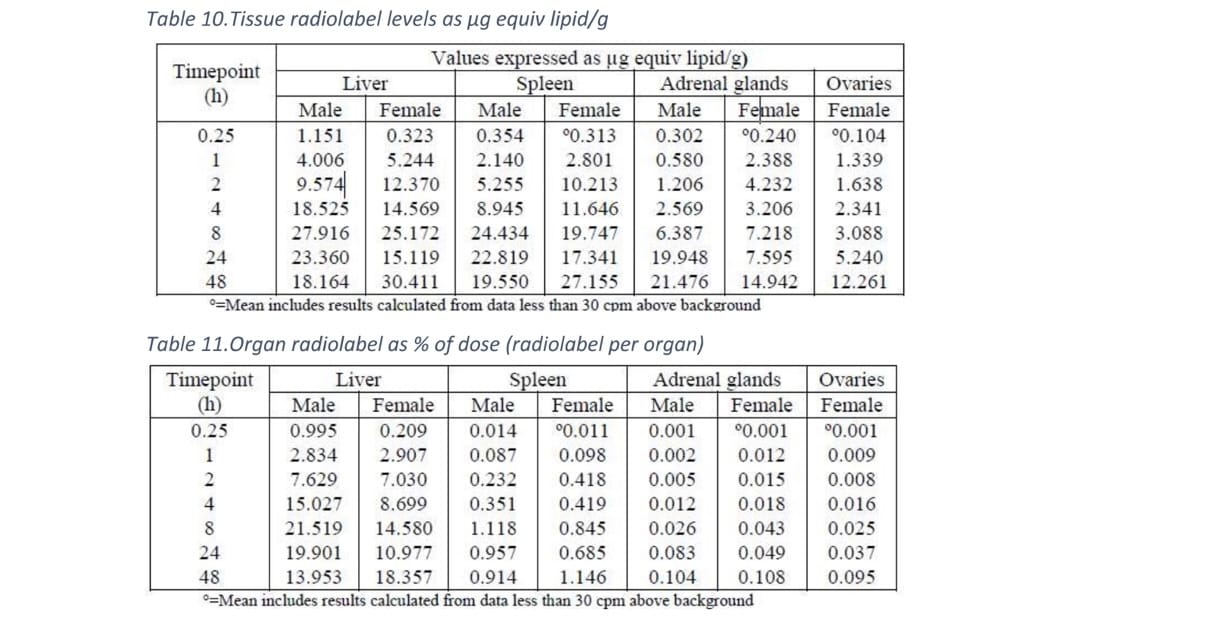
In its Non-Clinical Assessment, Medsafe evaluated a biodistribution study and observed that, “Over 48 hrs radiolabel [lipid] distributed to most tissues but only low levels were found in tissues other than the liver, spleen, adrenal glands and ovaries. The majority of the recovered radiolabel [lipid] was found in the liver as would be expected for a particulate, and the size of the organ, and to a lesser extent, the spleen. Tissue concentrations in the adrenals and ovaries were comparable to the liver and spleen however total recovery from these organs was low due to their comparative size. Levels in the liver and spleen peaked around 8 hours and at around 48 hours for the ovaries and adrenals.”
The report contains the following tables which set out distribution of the lipid to the liver, spleen, adrenal glands and ovaries at timepoints during the first 48 hours following vaccination:
In affidavit evidence given last year, Chris James the Group Manager of Medsafe, confirmed his knowledge of the biodistribution of the vaccine. James stated, “Pfizer provided this [biodistribution] study as part of its original application for the parent product. It was assessed, along with other non-clinical data, as part of Medsafe’s non-clinical evaluation of the parent product. No major concerns were raised that necessitated a request for additional information or condition of provisional consent. This is consistent with the assessments conducted by other regulators, see for example the European Medicines Agency’s assessment.”
James went on to state that one of the main concerns from the applicants in that court case, “seems to be that this study demonstrates that the LNP does not remain in the shoulder muscle but rather spreads through the body. However, it is not clear from Dr [X]’s affidavit why he considers that is cause for concern. This study does not show that the mRNA component (the vaccine) follows the same distribution pattern. Dr [X] also does not explain why it could be concerning for mRNA to spread in the body.”
As it was pointed out to the Court and Chris James in an affidavit from an expert in response: “This contradicts public messaging which suggested that a dose of Comirnaty would largely remain at the injection site, with some being taken by the cells of the immune system to the local draining lymph nodes where an immune response would be initiated. Indeed, this is how traditional vaccines work. It is concerning that public health officials did not reveal this atypical feature of Comirnaty.”
Indeed the Immunisation Advisory Centre (IMAC) website (which is run from the University of Auckland), still describes the vaccine working in a manner which is demonstrably incorrect by omitting to note that the vaccine is distributed through the body before degrading. The website currently states: “After injection, the mRNA contained within its lipid bubble is taken up by specialist immune cells (dendritic cells) in the muscle near the injection site. Using our cells’ own protein-making machinery, the mRNA provides the recipe to make a new protein that is known to trigger a good immune response. As normally occurs in our cells, after the protein has been made the RNA is broken down and its components are recycled – its job is done.”
Professor Nikki Turner is an advisor to IMAC and is also on multiple national advisory groups for immunisation clinical and policy issues including COVID vaccines for the NZ government, Ministry of Health and Pharmac. Until 2020 she was a member of the World Health Organization Strategic Advisory Group of Experts (SAGE) on Immunisation. Most notably, Turner succeeded Sir David Skegg as Chair of the Strategic Covid-19 Public Health Advisory Group which provides advice direct to the Minister for Covid-19 Response.
Reproduction and development
The Medsafe Non-Clinical Assessment notes that, “to a large extent the expanding clinical experience with the proposed vaccine has overtaken the nonclinical data and provides a more robust basis for assessment of most potential clinical risks. Areas where this is not the case include reproductive and developmental toxicity and the potential for genotoxicity and carcinogenicity.”
Medsafe records that as part of its evaluation of the vaccine, the European Medicines Agency asked Pfizer to discuss, “the concentrations of lipids in the ovaries over 48 hours, the precise location of the labelled lipid in the ovaries and the clinical relevance of this finding.” The EMA added that, “another discussion regarding the toxicity of this finding on fertility is also expected.”
Pfizer responded that, “in the developmental and reproductive toxicity study in rats there were no vaccine-related effects on female fertility or pregnancy, or embryo-fetal or offspring development.”
“No work has been carried out to understand the precise cellular location of the lipids (or any other components of the LNP) in the ovaries. Given the nature of the radiolabel detection methodologies, such precise cellular localization of the radiolabel is not possible. Only a small amount of the total dose that was administered to rats was present in the ovaries (0.1% of the dose). Most of the LNP remained at the injection site. In the repeat-dose toxicity studies, there was no evidence of vaccine-related macroscopic or microscopic findings in the ovaries.”
Medsafe considered this response from Pfizer to be “reasonable” but it did conclude that, “The proposed data sheet notes that there is limited experience in pregnant women and provides appropriately cautious advice that, ‘Administration of Comirnaty in pregnancy should only be considered when the potential benefits outweigh any potential risks for mother and fetus.’”
Medsafe’s view was that, “although not directly addressable from the nonclinical data, there may be a basis in the current circumstances for concluding the risk of vaccination during pregnancy is outweighed by the potential benefits of immunity particularly for specific subpopulations at heightened risk.”
Medsafe added that, “This is a clinical consideration but there is no nonclinical data that would preclude or limit this consideration.”
In other words, although there may not be direct evidence from non-clinical studies (animal studies), Medsafe believed that there may be a basis for concluding that the benefits of vaccination during pregnancy outweigh the potential risks, particularly for certain high-risk subpopulations. The Medsafe assessment does not, however, explicitly conclude that the benefits of vaccination outweigh the potential risks for all pregnant women.
Importantly, this statement indicates that Medsafe considered that weighing the potential benefits and risks of vaccination during pregnancy was a clinical consideration, i.e. a consideration to be made by healthcare professionals such as doctors, nurses, and other medical personnel in the treatment of individual patients.
Medsafe’s assessment indicates that there is no evidence from non-clinical studies that would suggest that vaccination during pregnancy should be avoided or limited. This suggests that, while more research may be needed, the available non-clinical data does not contradict the potential benefits of vaccination during pregnancy particularly for certain high-risk subpopulations.
However, shortly after the vaccine was given provisional approval, the Medical Council issued guidance to all GPs which instructed doctors to only discuss the benefits of vaccination. It did not state that GPs could discuss risks, uncertainties or alternatives which would usually be part of an informed consent discussion and which would be unique to each individual.
The Medical Council guidance concluded by warning that there, “was no place for anti-vaccination messages in professional health practice, nor any promotion of anti-vaccination claims including on social media and advertising by health practitioners”.
Despite numerous requests, the Medical Council has been unable to define what advice would be considered “anti-vaccination” and what advice would be considered appropriate and in accordance with the Medical Council’s existing guidance on informed consent which includes “highlighting risks specific to your patient”.
In contrast to the cautious approach set out in the Medsafe Non-Clinical Assessment which highlights the need for clinical consideration, IMAC’s advice to pregnant women, as set out on its website, is that “Vaccination against COVID-19 is recommended for pregnant people at any stage of pregnancy.”
Similarly, IMAC’s advice to healthcare professionals is that, “Vaccination is highly recommended during pregnancy, especially for those with underlying health conditions or high risk pregnancies.”
Impact
The Australian TGA Non-Clinical Assessment was made public within the last month after a lengthy Freedom of Information Act battle. The document was submitted to Medsafe in late January 2021 and contains comparable biodistribution studies indicating extensive distribution of the LNPs in major organs of the body, as those presented in the Medsafe Non-Clinical Assessment.
Medsafe has yet to release its Non-Clinical Assessment in full to the public, despite its high relevance to healthcare professionals and the public.
The report contains information that was relevant to members of the public and mandated workers when they were providing informed consent. To the extent that the risks, benefits or uncertainties of the vaccine were not accurately described to the public by health officials and members of the government, it could impact the validity of informed consent and could potentially constitute a breach of the Medicines Act 1981.
Furthermore, any material misrepresentation of the risks, benefits or uncertainties of the vaccine could have an impact on the various court cases that have considered the lawfulness of the mandates that were imposed on a number of workforces over the last 24 months. Those cases considered whether the relevant vaccine orders were a reasonably justifiable limitation on the right to refuse medical treatment under section 5 of the Bill of Rights Act 1990.
In NZDSOS Inc v Minister for Covid-19 Response, Justice Cooke noted that the right in section 11 to refuse medical treatment, “is well recognised in both legal and medical terms as being fundamental. It is associated not only with the concept of personal autonomy that is at the heart of the relationship between the state and the individual, but also the concept of informed consent that is deeply embedded in the principles of medical ethics and practice. It is true that the vaccinators involved in the nationwide vaccination programme should still have observed the principles of informed consent when administering the vaccine. But the pressure created by the mandates, and the general circumstances, have plainly reduced the significance that is otherwise so strongly placed on informed consent … What this means is that there is a very significant evidential burden placed on the Crown to demonstrate that the measures implemented by the Order are reasonable, and demonstrably justified in a free and democratic society.”
If a Court were to find that misrepresentations relating to the benefits or risks of the vaccine were material and that they could have affected the decision-making of those who were subject to the mandates, it may conclude that the mandates were not justified after all.
My article relating to Medsafe’s approval process is here.
My article relating to Medsafe’s approval of the vaccine for 12 to 15 years olds is here.
My article relating to the government’s knowledge of the myocarditis risk is here.







{kind=link}