
Table of Contents
Megan Mansell
Megan Mansell is a former district education director over special populations integration, serving students who are profoundly disabled, immunocompromised, undocumented, autistic, and behaviorally challenged; she also has a background in hazardous environs PPE applications. She is experienced in writing and monitoring protocol implementation for immunocompromised public sector access under full ADA/OSHA/IDEA compliance. She can be reached at MeganKristenMansell@Gmail.com.
Many public health responses we saw during the pandemic were inherently unethical, but our flippancy concerning child safety in public schools has been among the most egregious. Sadly, families remain largely resourceless against power-hungry leadership.
Masking remains an issue hotly debated at school board meetings around the globe. In Ontario, Canada, on November 24th, 2022, a district-wide mask mandate was narrowly avoided by a 6-6 vote. While parents were relieved, it was too close for comfort.
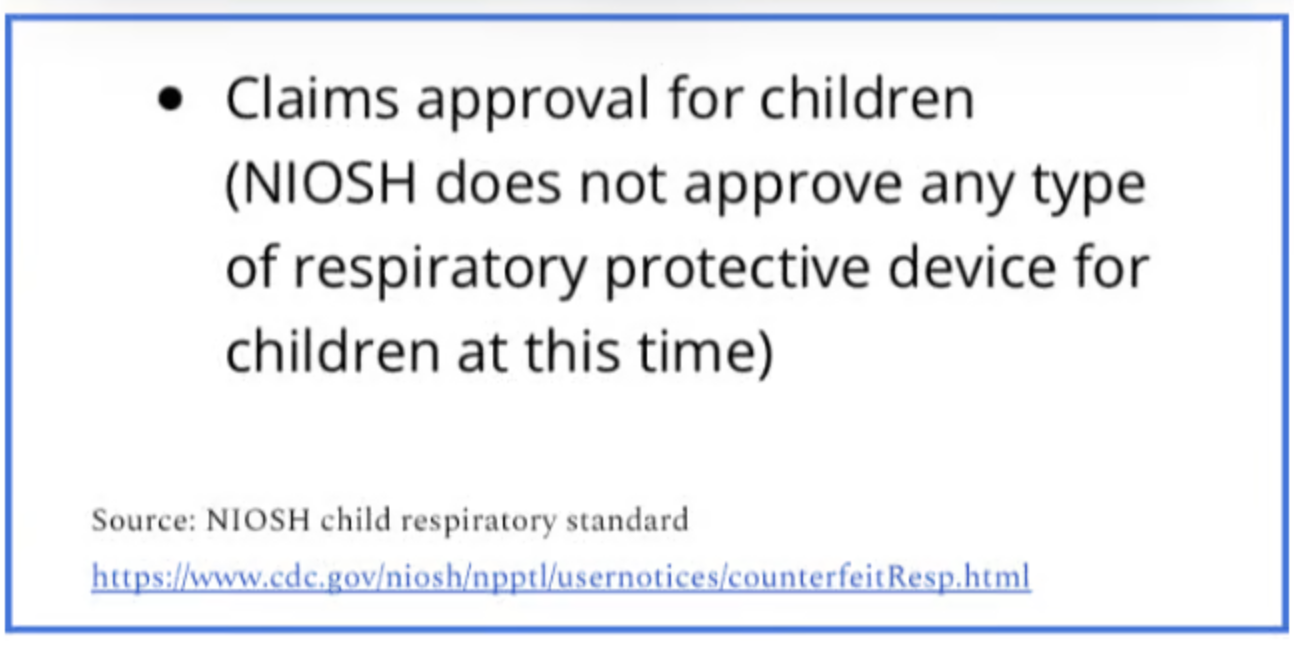
It begs repeating, and with great emphasis, that every mask you have ever seen on a child is unregulated, untested, and unsafe, with zero efficacy, fit, term of wear, or medical clearance standards. Zero.

In school settings, teachers and staff taking the place of parents is termed In Loco Parentis – yet the denial of medical autonomy has just been muy, muy loco. It is absurd to pretend that In Loco Parentis means that the school suddenly gets to make medical decisions on behalf of a minor child, including decisions regarding respiratory protection.
Were a student critically injured while on campus, medical professionals would make relevant decisions until a parent was present, never asking a teacher, principal, or superintendent to make healthcare choices. Were a teen to fall pregnant, a teacher cannot consent to an abortion in place of a parent. A school nurse is a caregiver, not a guardian. This is a line we cannot allow to be blurred.
In the instance of masks, children are in something for 8-12 hours per day that is not approved for extended wear even in adults. Adults must undergo exhaustive medical clearance and extensive fit testing before donning hazard-specific, Industrial Hygienist-prescribed kit under specific terms of wear. Workplace respiratory protection programs necessitate filtered supplemental air to account for respiratory interferences from extended periods of restricted breathing.
Other hazards, such as inhalation of loose fibres and exposure to the vast microbial accumulation found on masks are other considerations given in respiratory protection evaluations. Over time, masks become a living medium in a warm, moist environment. While dentists and surgeons do wear masks to prevent splatter and spray from entering oral and nasal mucosa, they do not keep wearing them all day, breathing in disgusting microbial souvenirs. They most certainly do not wear surgical masks for mitigation of airborne pathogens – unless they want to be exposed.
We skipped that necessary medical clearance and consent arm of respiratory protection with children. We require rigorous safety standards from all other child-related products.
Why would we ignore safety protocols for something with known, anticipated harms?
Simply calling something unethical is a far cry from proving it to be so. By mapping out the specific details of demands like compulsory masking, we can push for these practices to be argued before Institutional Review Boards (IRBs) for human studies to prove the unethical nature of our policies. I created a replica study of school-based masking practices for doctors to bring before their IRBs, the correct domain for such a debate, as opposed to school board meetings. Perhaps we can finally put an end to these inhumane practices before things escalate to irreversible harm.
I had a doctor argue my replica study before her IRB in Arizona, and it was unanimously rejected based on extensive ethical violations and anticipation of harm.
From the IRB meeting minutes, “A study was brought before this IRB. It was noted that the proposed study would introduce risk to children. It seemed to the group that we are rejecting this on the basis of violation of First Do No Harm. There would be no medical supervision during this time, even if children were severely impacted physiologically during wear. Frightening. A motion was made: Reject this study because the children would not be assessed medically, and it violates Primum non nocere. And it is unethical. The motion was seconded. The motion then passed by unanimous vote to reject this study on ethical grounds.”
Their reaction thoroughly sums up my objections with these practices.
Replica Study (exact wording as presented)
In a proposed replica study of what schoolchildren are experiencing on a daily basis due to mandated masking, a few design elements would be critical.
The masks seen on children are unregulated, untested, and without efficacy standards for particle grade. There exist no fit or safety standards for extended wear, no qualitative fit testing as is standard with workplace apparatus requirement, and no monitoring of health status including physiologically impacting interferences such as deoxygenation, hypercapnia, or linguistic and developmental interferences from being unable to see tooth, tongue, and lip placement. The apparatuses seen on children are expressly non-mitigating for aerosols by OSHA and NIOSH standards, wherein an apparatus must be 90% effective to be considered mitigating and 3.2% leakage equates to 100% inefficacy for aerosol exposure.
So in a study focused on child participants, the behavioural ramifications of noncompliance would need to be universal; noncompliance for wearing the apparatus would result in punishment such as the loss of preferred activities or running laps masked during recess, as is commonplace in our school systems.
Oxygen levels could be monitored, but children would be required to wear them even if their oxygen levels decrease into unsafe levels during wear (as there has been no health monitoring provided in schools).
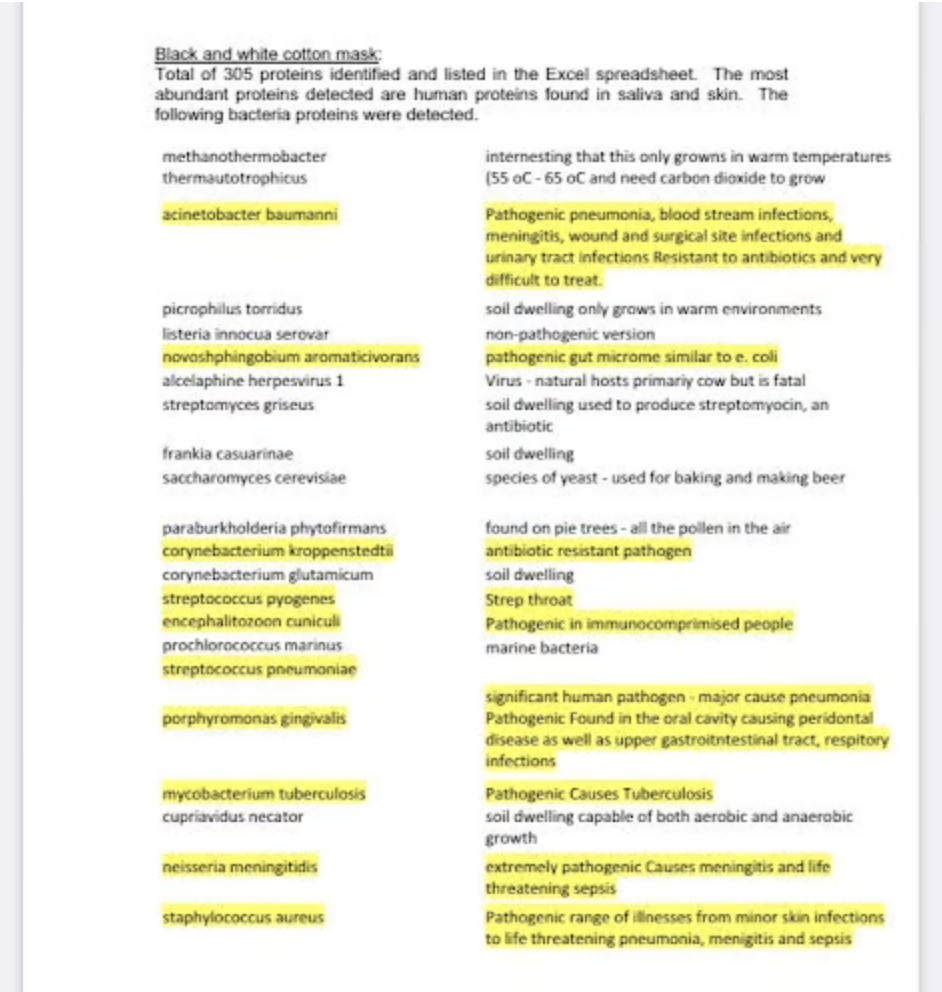
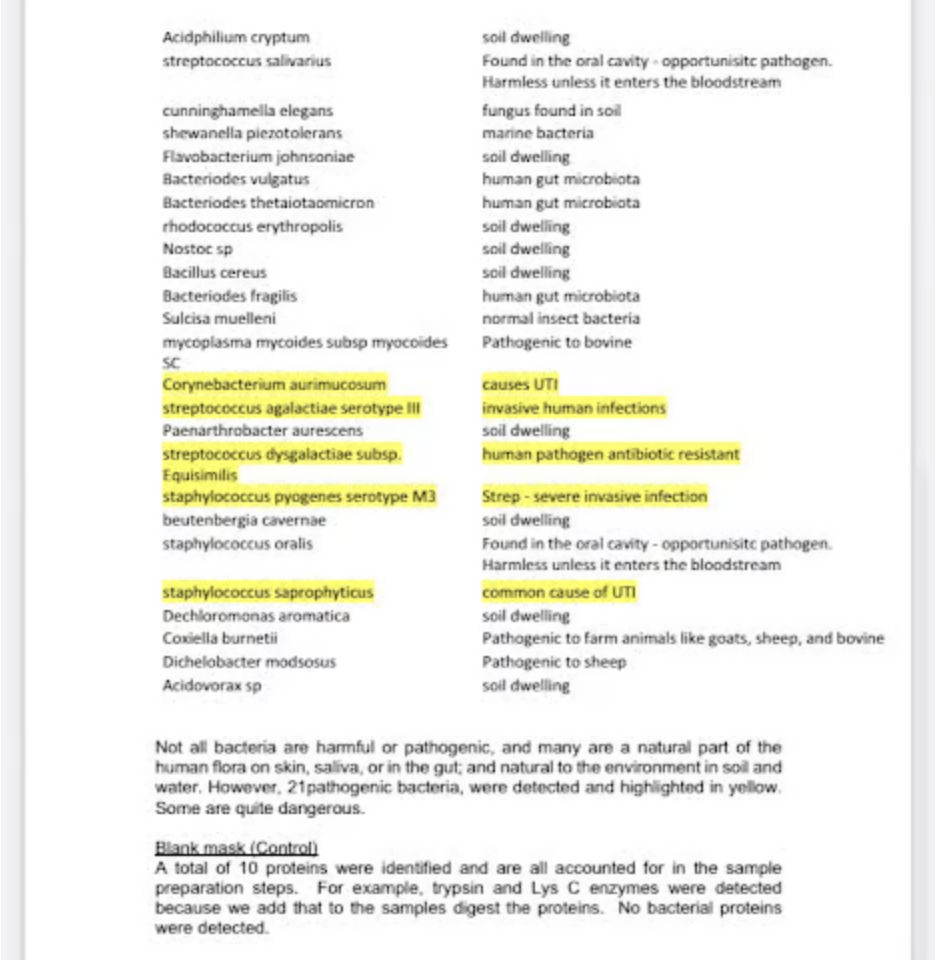
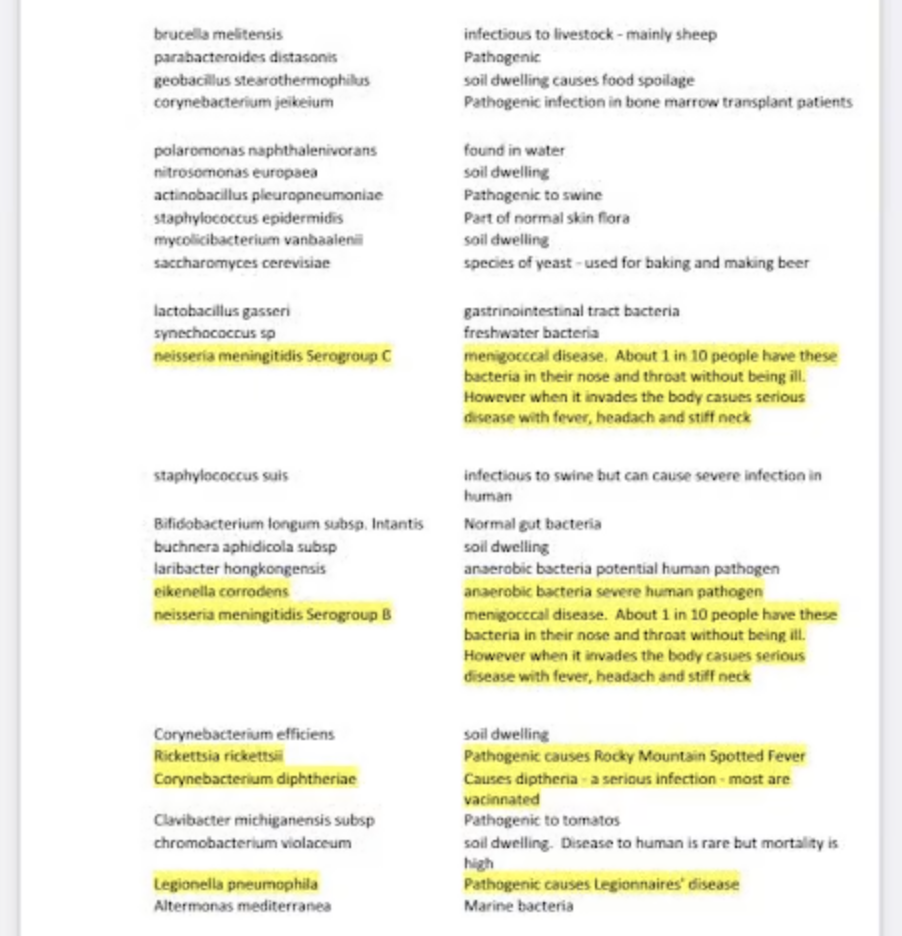
There would be no medical clearance aspect, so students would be required to wear these apparatuses even if severely impacted in a physiological capacity during wear. The attached 3 pages of pathogenic findings are from one day of wear; test subjects would be in a non-sterile environment, potentially exposed to the gamut of pathogens listed below, and children who drop their masks or set them down in unsanitary places would be required to keep wearing the mask on for the duration of the day.
Children in school systems wear masks for 8-12 hours per day, so in summary, we would have unregulated apparatuses on children with no medical clearance or parental consent, with no regard given for deoxygenation or hypercapnia observed in study participants, harsh penalties for noncompliance, and exposure to dangerous pathogens directly in front of oral and nasal mucosa in a warm, moist environment prime for biological amplification for 8-12 hours per day. It would be important to show the longitudinal impact of physiological and developmental interferences, so the study would need to be at least 1 year minimum.
Considerations
If our leadership took public health messaging seriously, they would be painstakingly specific when educating the public during a crisis. For the medically vulnerable, we must prevent instilling a false sense of security, especially when following a given measure will likely result in susceptible individuals being harmed or killed.
A similar study design is due for elderly and medically vulnerable populations. If an individual has a history of respiratory conditions, we should seek focused protection measures that do not exacerbate underlying issues; we must not implement compulsory use of methods that are harmful and do not work.
Have those pushing increasingly restrictive apparatuses on children even stopped to consider the reality of what children are experiencing on a minute-by-minute basis? Children depend on us to provide safe educational settings, with make-believe reserved for play, absent from our methods of protecting the medically vulnerable. Yet in terms of schools and proper mitigation efforts, we failed them all.







{kind=link}