Table of Contents
Our leaders should examine accumulated data to see what has actually happened, not what the models predicted. Look at empirical evidence and the fundamental principles of biology and then get the economy going again.
Level 3 (or Level 4 with KFC as Judith Collins labelled it) has been generously dangled in front of us by “Dear Leader” Jacinda Ardern but many are asking why not Level 2 (or even Level 1) for some areas. As ExPFC pointed out:
What this list shows is there are quite a lot of regions that haven’t had any confirmed cases for quite some time. Taranaki hasn’t had a confirmed case reported since the 1st of April, Hutt Valley since the 2nd of April, Nelson Marlborough since the 5th of April and Waikato since the 11th of April. The cases for West Coast and Wairarapa are so old they aren’t even on the list anymore.
It seems that those totally controlling our lives at present are ignoring some obvious conclusions.
The risk of dying from COVID-19 doesn’t seem as bad as we were told.
The numbers in New Zealand are very small so extrapolation is fraught with issues but so far 18 have died from 1461 confirmed and probable cases. That is 1.2%
Overseas the numbers are much lower. A recent Stanford University antibody study now estimates that the fatality rate if infected is likely 0.1 to 0.2 percent.
Based on the large data set in New York City, the rate of death for people 18 to 45 years old is 0.01 percent. In the older age group 75+ the NY rate is 0.8% which is closer to the NZ figures.
A significant factor everywhere appears to be comorbidity and while we have not had all the data released here in New Zealand, what we have been told bears that out. Certainly, in NY the figures indicate that to be true. 6,520 out of the fully investigated 6,570 COVID-19 deaths (99.2 percent) had an underlying illness.
Without an underlying chronic condition it appears that your chances of dying are small regardless of age, with young adults and children in normal health in the ‘almost no risk’ category.
Protect the older and at-risk people to eliminate hospital overcrowding.
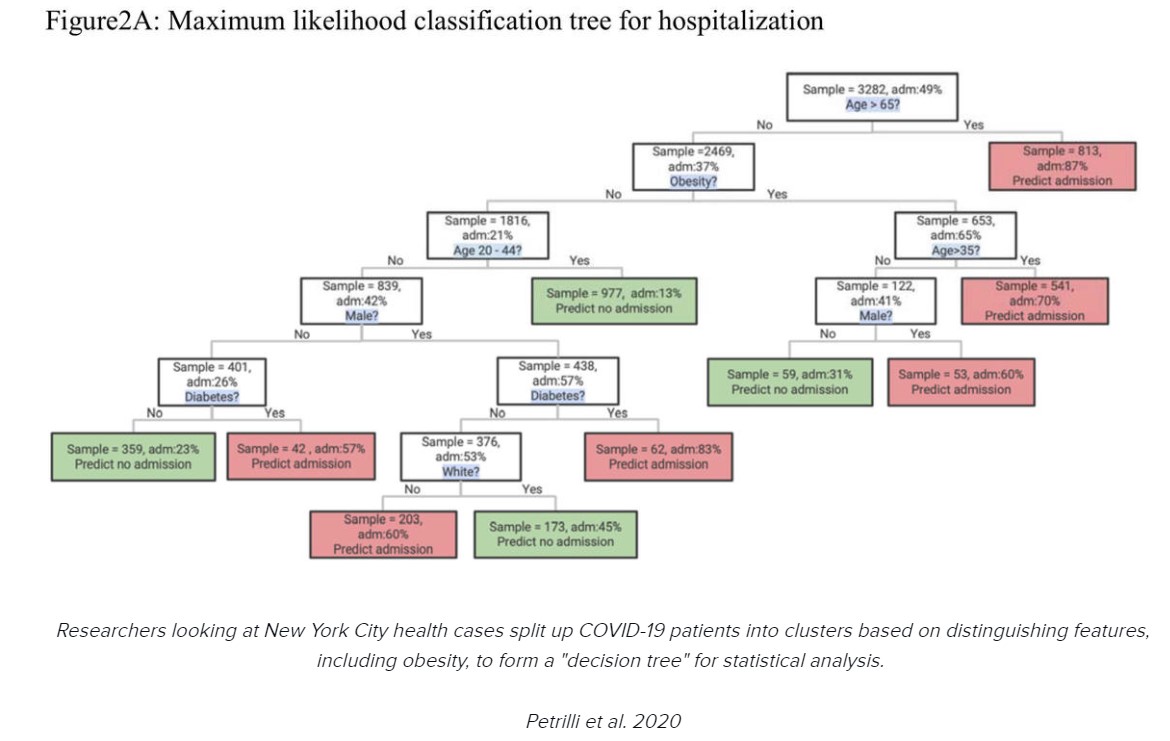
Based on the largest case series from the United States to date Petrilli et al found that an accurate predictive model for hospital admission could be constructed. After age, the factors are obesity, male sex, diabetes and white race.
Protect the at-risk and let the rest get on with life.
We cannot achieve herd immunity in our bubbles.
We all know from decades of medical science and experience that by transmitting the virus to others in the low-risk group who then generate antibodies, they block the network of pathways toward the most vulnerable people, ultimately ending the threat. Extending whole-population isolation directly prevents that herd immunity from developing.
People will die because other medical care is not getting done.
What will be the long term effect of the cessation of cancer screening, biopsies of tumors now undiscovered and so forth?
Mike Keaney knows his prostate cancer is a ticking time bomb. He was scheduled to have surgery on April 1 at Palmerston North Hospital, but it was cancelled as resources were prioritised in response to Covid-19.
msn.com/en-nz/news/national/cancer-sufferer-in-limbo
As Dr Scott W. Atlas, the David and Joan Traitel Senior Fellow at Stanford University’s Hoover Institution and the former chief of neuroradiology at Stanford University Medical Center, has pointed out:
The overwhelming evidence all over the world consistently shows that a clearly defined group — older people and others with underlying conditions — is more likely to have a serious illness requiring hospitalization and more likely to die from COVID-19. Knowing that, it is a commonsense, achievable goal to target isolation policy to that group, including strictly monitoring those who interact with them. Nursing home residents, the highest risk, should be the most straightforward to systematically protect from infected people, given that they already live in confined places with highly restricted entry.
The appropriate policy, based on fundamental biology and the evidence already in hand, is to institute a more focused strategy like some outlined in the first place:
- Strictly protect the known vulnerable,
- self-isolate the mildly sick and
- open most workplaces and small businesses with some prudent large-group precautions.
This would allow the essential socializing to generate immunity among those with minimal risk of serious consequence, while saving lives, preventing overcrowding of hospitals and limiting the enormous harms compounded by continued total isolation. Let’s stop underemphasizing empirical evidence while instead doubling down on hypothetical models.
The Hill
So why can’t the regions identified by ExPFC be sent to Level 2 or 1 instead of the long drawn out nationally imposed descent into economic carnage? The Levels are allowed to be applied regionally.
If you enjoyed this BFD article please consider sharing it with your friends.








{kind=link}