Table of Contents
Ani O’Brien
Like good faith disagreements and principled people. Dislike disingenuousness and Foucault. Care especially about women’s rights, justice, and democracy.
I genuinely didn’t know what I was looking for when I went searching through FYI.org on Friday night. I was confused by timelines that weren’t making sense and increasingly implausible deniability.
Why were we talking about whether the Covid-19 Response Minister Chris Hipkins knew about the risks of double-dose vaccination of young people in March 2022 when the risk of myocarditis in young people, particularly after a second dose, was already being formally discussed and managed within the government health system at least eight months earlier? How could Chris Hipkins have lived and breathed our Covid-19 response and been completely unaware of whether there was any truth to one of the most often spoken about claims about vaccine harm? How could he have been confident in refuting what he called “misinformation” if he had never inquired with experts about whether it was true?
Chris Hipkins has repeatedly claimed ministers were not aware of this advice at the relevant time. However, a cabinet paper in his name from March 2022 includes the advice and made the front page of the New Zealand Herald on Friday. Specifically, the dispute now centres on advice that a two-dose schedule for under-18s may have added unnecessary myocarditis risk and was not justified by transmission risk for this population.
The timelines and lack of knowledge of key ministers just didn’t seem right. So I typed “myocarditis” into FYI.org and scrolled aimlessly through Official Information Act requests from 2021 and 2022. I clicked into anything remotely related to young people. There were quite a few…
If ministers genuinely didn’t know something this important we would expect to see gaps in the paper trail, an absence of the information, but that isn’t what I found. Quite quickly, the records I sifted through showed the information (that the Covid-19 response minister was apparently oblivious to) moving through the health system, being discussed in documents written by a variety of different people. What the Official Information Act documents show is not absence of knowledge, rather a system actively engaging with myocarditis risk in young people long before the 9 December 2021 Covid-19 Vaccine Technical Advisory Group (CV TAG) advice that Hipkins and Verrall claim not to have been given. That does not automatically prove ministers saw the December advice when it was written, but it does make total ignorance of the underlying risk much harder to believe.

The real timeline begins as early as July 2021. In a formal memo to then-Director-General of Health Ashley Bloomfield on 21 July 2021, CV TAG stated that emerging data indicated a risk of myocarditis and pericarditis following mRNA vaccination, and that the risk appeared to be higher following the second dose, in males, and in younger age groups.1 The memo went further, quantifying the risk from overseas data and recommending that people aged 16 to 29 receive their second dose at least eight weeks after the first, and that people aged 12 to 29 under cardiology review discuss the risks and benefits with their healthcare team. This was formal advice to the director-general identifying a dose-specific risk pattern in younger populations.
By that point, concerns about myocarditis were also not fringe speculation, they were already being explicitly raised within New Zealand’s own advisory ecosystem. In a 6 July email, a senior advisor in the Office of the Children’s Commissioner (OCC) sought information so that she could respond to correspondence and refers directly to “rarer effects… eg myocarditis and pericarditis… that can cause death or long term ill health”.2 In response, a paediatric consultant, senior lecturer, and advisor to the Immunisation Advisory Centre (IMAC) responded reassuring that the vaccine is “not experimental” and “in NZ Medsafe has preliminarily also approved this Covid vaccine for this age group 12-15 yrs based on evaluatig [sic] the safety and efficacy information.” However, she also says “side effects are more common in younger people and children” and that “general [side] effects were more common after the second dose than first dose.”
The OCC advisor is effectively checking with a medical expert as to whether some of the concerns and claims being put to the OCC are credible. The doctor’s response is emphatically confident in the vaccine, but she is not ambiguous nor hesitant in acknowledging that children and young people are affected differently to adults and that the second dose presents more side effects. This was clearly not hidden knowledge, nor some late-breaking discovery.
Around the same time, the same OCC advisor approached other experts about similar concerns being raised with the Children’s Commissioner.3 These related to the impacts of vaccines and lockdowns on children. She explains “we are starting to receive letters to the OCC opposing vaccination of children from scientists and clinicians, not just worried public…” In response, epidemiologist and clinical paediatrician Dr Amanda Kvalsvig also endorses that “vaccinated children are experiencing better outcomes than children with Covid-19 infection”, but shares that:
A recent US case series reported a finding of myocarditis and/or pericarditis (they are hard to distinguish) in seven adolescents (all male) aged 14-19 years who had been vaccinated. This finding has sparked a discussion about whether vaccination caused the myocarditis or whether it was coincidental… As a result of this report, instances of myocarditis or pericarditis are being closely monitored in the adolescent US population and elsewhere…
In other words, the issue was well known in medical circles in July 2021. It was being studied and monitored around the world. Dr Kvalsvig was one of the most prominent voices from medical academia during New Zealand’s Covid-19 response. She has co-authored papers with Dr Michael Baker and is quoted in many news articles throughout the pandemic. The point is not that Amanda Kvalsvig briefed ministers directly. It is that a prominent public health voice was openly discussing myocarditis risk in adolescent males at the same time official advisory bodies were doing the same internally. The idea that this issue existed everywhere except the ministerial orbit is increasingly implausible.4
By August 2021, this knowledge had moved beyond background concern and into the formal policy process. Minutes from the Immunisation Implementation Advisory Group (IIAG), a body feeding directly into government decision making, show that when officials were considering extending vaccination to 12–15-year-olds, they explicitly noted “the concerns around myocarditis in younger males”.5 Specifically named in the minutes as responsible for this section was Allison Bennett, Public Health System Group Manager, Ministry of Health. The same section also noted:
The Ministry has received technical advice from CV-TAG following the Medsafe ‘decision to use’ Pfizer for 12-15-year-olds. Current thinking is the extension in the first instance could apply to ‘at risk’ members of this age group.
Around the same time, a 4 August 2021 CV TAG memo on priority groups for 12–15-year-olds explicitly recorded that children and young people had a low risk of severe disease or death due to Covid-19, that vaccination should not yet be routine for all in that age group, and that broader use would depend on further evidence, including the incidence, risk factors and outcomes of myocarditis after vaccination in adolescents.6
This is quite significant. The government was actively weighing whether to use Pfizer to vaccinate children at all, and myocarditis risk was part of that discussion. Risk-benefit decisions depend on both sides of the equation. If Covid risk is low, even a rare vaccine side effect carries more weight. I find it very difficult to believe that this very important trade-off consideration, which led to them at least initially suggesting that only “at risk” young people get vaccinated, was not on the minister’s radar. Even if we accept that these highly qualified and clearly fastidious officials did not think to mention to the minister that they were weighing up the risk of vaccinating “at risk” young people versus all young people, is it likely that the minister still did not know some five or six months later in early 2022?
These minutes alone undermine any claim that the issue of risk to young people had not been identified or considered at the time decisions were being shaped. Is Chris Hipkins lying then? Or was he so detached from the actual decision making that he was allowing officials to run the show while he did press conferences?
By October 2021, the situation had progressed even further. Minutes from a CV TAG meeting refer to an update from the Science and Technical Advisory (STA) on myocarditis:7
An update was provided from STA on the risk of myocarditis according to international evidence. Data presented at the latest US ACIP meeting on 30 August 2021 and data from Israel indicate that myocarditis reporting rates following mRNA Covid-19 vaccination continue to be rare overall, but highest risk tends to occur after the second dose, particularly in younger males.
The minutes reflect that they discussed that they are expecting long-term data at the end of November. This demonstrates that myocarditis was not simply an identified risk. It was a standing agenda item, a quantified issue, and an operational one.
Most tellingly, officials note that information on symptoms of myocarditis had already been distributed to vaccinators. Does this mean we are supposed to believe that important information about a serious (but rare) side effect was communicated to everyone except the minister in charge of the entire response?
Come on. You do not issue clinical guidance, track dose-specific risks, and brief frontline staff unless you have accepted that a side effect is real and requires active management. And if it needs active management the minister should know about it because he is making the decisions around whether to make it mandatory for anyone, but especially under-18s to have a double dose.
In the 2 November 2021 CV TAG minutes, they formally discussed a long-term follow-up study of myocarditis and pericarditis cases following vaccination in the New Zealand population:
A request to support research myocarditis following Covid-19 vaccination was also considered...8
You don’t consider commissioning long-term follow-up studies for something you consider negligible. That is what systems do when they regard a risk as real enough to warrant structured investigation.
These documents do not contain smoking guns that say that the vaccine was totally unsafe and should not have been used. The medical professionals involved clearly support the use of the Pfizer vaccine. What is important here is that the government mandated it. And if the government is going to force a medical treatment on people and take away their ability to make informed (or ill-informed) decisions about their health and their children’s, then the bar is even higher for safety.
We take medications all the time that have side effects and serious risks, but usually we are able to make the choice to do so along with receiving personalised advice from our doctor. When the government decided, led by Jacinda Ardern and Chris Hipkins, to make blanket mandates requiring double vaccination for everyone aged over 12 years, they took away that choice. These are policy settings that effectively required double vaccination for over-12s in order to access large parts of public life. It is reasonable, therefore, to expect that they were completely across the risks they were signing us all up to. Especially when it came to our children.
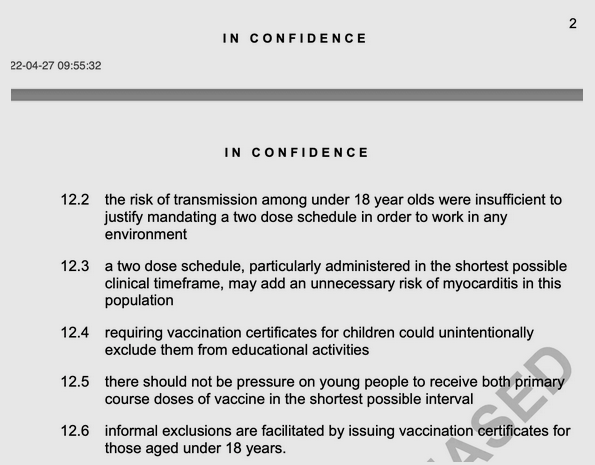
As we now know, by March 2022, concern had reached cabinet-level material in plain terms. In the paper signed by Hipkins on the implementation of the paediatric vaccination programme, officials recorded that the individual health risk of Covid-19 to under-18s was low, that the risk of transmission among under-18s was insufficient to justify mandating a two-dose schedule, and that a two-dose schedule, particularly administered in the shortest possible clinical time frame, may add an unnecessary risk of myocarditis in this population.9
It is is reasonable to expect that they would communicate those risks.
This all creates a timeline that is difficult to reconcile with the public narrative we’ve been fed by Chris Hipkins since the Royal Commission Phase Two report was published. He has sworn in parliament and to the media that he had no idea of the risk to young people when he mandated the double dose of the vaccine. Internally, the system was identifying myocarditis risk in at least early July 2021, incorporating it into policy discussions by August, and managing it operationally by October. And yet, Hipkins tells us he did not know. He says the Ministry of Health did not brief him.
At minimum, the documents show that the ministry and its advisory bodies were grappling with this issue long before December 2021. The remaining question is whether that knowledge failed to reach ministers, or whether ministers are now pretending it didn’t.

Chris Hipkins’ defence has shifted slightly in the past day or two. He now says:
While I do not recall all of the advice we were provided over the three years, ministers kept the vaccine mandates under review and continuously sought expert advice on the safety and impact of vaccinations for under-18s.10
Hang on. If ministers were continuously seeking expert advice on safety, then myocarditis, a risk already identified, tracked, and formally discussed within the system, should have been front and centre. He cannot claim both active oversight and total ignorance.
The cabinet paper in his name shows he knew in March 2022 and yet did not immediately lift the mandate or advise the public. If he didn’t know even then, as he seems to be alleging in some comments to media, someone was writing cabinet papers for him (likely) and he was submitting them without reading (unacceptable).
So when he stood up on 6 April 2022 and celebrated free boosters (a third dose) for 16- and 17-year-olds, it followed a cabinet paper in his own name that had already acknowledged the low Covid risk to under-18s, the lack of transmission justification for a two-dose requirement, and the possibility of unnecessary myocarditis risk in this population.11
In recent weeks, Hipkins has repeatedly stated that he would have taken action or acted differently had he received the advice sooner, but he did have the advice in March and he promoted an additional (third) dose for young people.
A few days ago he told media:
[The March 2022 Cabinet paper] doesn’t materially change what Royal Commission [sic] found. It doesn’t materially change the concern at the time, which is that that advice around myocarditis risk should have been presented to ministers when we were making those decisions around mandates and around requirements.12
For his claims of ignorance to be true, multiple things would all have to fail simultaneously. Either the advice never left the advisory layer (STA and CV TAG), or it was actively filtered out before reaching ministers (by MOH/Dr Bloomfield?), or ministers ignored or didn’t read briefing material tied to cabinet decisions.
The system would have had to be in a full-blown conspiracy to keep the information from him or it is evidence that he was nothing more than a bloke on a stage making jokes about spreading your legs while the people behind the scenes made all of the decisions.
No scenario is good.
These were not isolated academic observations buried in obscure correspondence. They were discussed in advisory groups, incorporated into official minutes, and translated into operational guidance. CV-TAG and IIAG processes feed into ministerial briefings and when a risk is being actively managed at multiple levels of the system, it is not credible to suggest that those at the top were unaware of it.
What makes this even harder to swallow is the retrospective rewriting of history. We’re now told by Chris Hipkins that he never gave out medical advice and that it was down to doctors to advise patients about risks, as if New Zealanders were making fully informed, free choices. As if he didn’t stand on a podium almost every day and tell us when we were allowed to leave our houses and that we had to wear face masks into restaurants, but could remove them once seated.
Doctors who raised concerns about vaccine risks, including myocarditis, were publicly censured, professionally investigated, and in some cases lost their jobs or faced serious disciplinary action. At the same time, patients couldn’t just have a conversation and opt out anyway. They had to apply for formal exemptions through a tightly controlled process that overwhelmingly declined requests. Dissenting voices were shut down while the public was funnelled through a system designed to minimise scrutiny.
So where does this leave Chris Hipkins? Even the most generous interpretation that no single briefing paper landed on his desk spelling this out in bold with flashing neons signs does not resolve the problem. Ministers are not just passive recipients of isolated memos that they dutifully just sign off on. They are accountable for the systems they oversee and Chris Hipkins is accountable for the system he says kept this massive secret from him. “I didn’t know” is not a defence when the machinery of your government demonstrably did.
This is not a case of ‘hindsight is 20/20’. The documents show early awareness, ongoing monitoring, formal consideration in policy settings, and eventual operational response, before the public conversation caught up. The issue is not whether myocarditis risk existed (it did) or whether officials knew (they did). It is that the timeline presented to the public does not align with the timeline that can be found in the shallowest of dives into the documents.
By July 2021, officials had formally identified the myocarditis issue, quantified its age and sex pattern, and recommended a longer interval between doses for younger adults. By August, they were weighing myocarditis explicitly in decisions about whether to vaccinate children at all. By October and November, they were managing the risk operationally and considering long-term research. By March 2022, cabinet-level material acknowledged that under-18s were at low risk from Covid, that transmission risk did not justify a two-dose mandate, and that a compressed two-dose schedule might add unnecessary myocarditis risk.
They say it is never the ‘crime’ that gets you. It’s the cover up. And so it is true for Chris Hipkins in that this is no longer about a public health question (Should he have mandated double dose vaccination for 12-17 year olds?). It is rather a question of what his repeated claims to have not known about the risk that accompanied that mandate say about his willingness to be accountable, his honesty, and his integrity.
The paper trail shows that the risk was known earlier, discussed more explicitly, and managed more actively than has been publicly admitted. Whether that knowledge reached him through formal briefings, cabinet papers, or the wider system he was responsible for, the claim of ignorance is no longer credible.
He knew.
1 https://web.archive.org/web/20230320025727/https://www.health.govt.nz/system/files/documents/pages/20210721_-_cv_tag_myocarditis_following_vaccination.pdf
2 https://fyi.org.nz/request/16858/response/65685/attach/11/Paediatric%20epidemiologist%20email%202.pdf
3 https://fyi.org.nz/request/16858/response/65685/attach/5/Epidemiologist%20AK.pdf
4 https://newsroom.co.nz/2021/10/13/govt-shrugs-off-expert-pleas-for-level-4-expects-cases-to-spike/
5 https://fyi.org.nz/request/15571/response/68407/attach/4/Scott.OIA%20response%20H202114872%20part%201%20Copy.pdf
6 https://fyi.org.nz/request/16691/response/70341/attach/5/Appendix%201.pdf
7 https://fyi.org.nz/request/16691/response/66492/attach/3/H202115494%20Response.pdf
8 https://fyi.org.nz/request/16691/response/66492/attach/3/H202115494%20Response.pdf
9 https://www.health.govt.nz/system/files/2022-05/implementation_of_covid-19_pfizer_paediatric_vaccine_for_children_aged_5_to_11_years_report_back.pdf
10 https://www.nzherald.co.nz/nz/politics/chris-hipkins-says-he-never-got-the-unnecessary-risk-advice-on-teens-and-covid-vaccine-this-cabinet-paper-shows-otherwise/premium/QIIBV5UQNFDFVFCHY7VKXCGIJA/
11 https://www.beehive.govt.nz/release/young-people-aged-16-and-17-eligible-covid-19-boosters
12 https://www.stuff.co.nz/politics/360957046/chris-hipkins-says-advice-about-vaccine-risk-teens-arrived-too-late
This article was originally published by Thought Crimes.