
Table of Contents
Guy Hatchard
hatchardreport.com
Dr Guy Hatchard is an international advocate of food safety and natural medicine. He received his undergraduate degree in Logic and Theoretical Physics from the University of Sussex and his PhD in Psychology from Maharishi University of Management, Fairfield Iowa.
Information
Opinion
Warning
Long Read. 1350 words.
A paper published on April 5th in the New England Journal of Medicine entitled “Protection by a Fourth Dose of BNT162b2 against Omicron in Israel” is raising eyebrows in the scientific world because of its deficiencies.
Dr. Vinay Prasad is an American hematologist–oncologist and health researcher. He is an associate professor of Epidemiology and Biostatistics at the University of California, San Francisco. His work has coined the term medical reversal whereby more careful trials of a drug show that its earlier approval was flawed.
Dr. Prasad, who is not an anti-vaxxer by any stretch of the imagination, has aired his concerns about the latest Israeli paper on Omicron and boosters in a YouTube video titled: “Israeli Data for the 4th Dose | How Good Is It? | Make Bourla Earn His Pay.”
In essence, Dr. Prasad is concerned that there is a potential for inherent bias as the group of subjects in the Israeli study who took the fourth booster was self-selected rather than randomly assigned.
In other words, he was asserting that any assessment of vaccine efficacy published in a leading journal like the NEJM should use the gold standard of scientific proof, rather than inferior methods known to allow confounding effects to creep in.
Dr. Prasad pointed to the current $100 billion of annual Pfizer revenue and asked: Why isn’t Pfizer conducting randomised controlled trials to assess the efficacy and safety of boosters rather than applying political pressure to bypass scientific concerns? He said this was debasing scientific standards.
Dr. Prasad also pointed out that the actual data underpinning the results of the Israeli study were inconsistent with the known trajectory of immunity development and therefore with the study’s conclusions that the booster was helping.
So precisely how could self-selection in the Israeli study invalidate results? Dr. Prasad suggested one possible mechanism: those volunteering for fourth boosters might be more healthy individuals.
We ask: How could this happen? There are a number of ways.
For example, let us take seriously the commonly voiced proposal that the Covid-19 spike protein is essentially a toxin. A toxin capable of causing the heart and organ inflammation, neurological effects, and the potentially damaging immune system storm associated with both Covid infection and vaccination.
As with any toxin, some individuals will have greater and others lesser reactions to the toxin depending on a whole range of individual physiological circumstances.
As the series of inoculations proceeds from first to fourth jab, those individuals having a greater adverse reaction to the shots will be weeded out by self-selection.
Those experiencing more unpleasant reactions to the spike protein toxin will naturally decide to forgo further injections as the vaccination series unfolds.
Since both the Covid virus and the vaccine expose the physiology to the spike protein which accounts for a significant part of the Covid aetiology and symptomatology, those more tolerant of the toxic effects of the spike protein will have lesser symptoms following Covid infection.
The net effect of this on the results of the Israeli study is clear, those volunteering to receive the fourth booster will appear to be gaining benefit from the booster because they have self-selected for greater tolerance.
As a result, there will be a tendency to see a slightly lower rate of hospitalisation and death subsequent to receiving the booster, precisely the result of the Israeli study. As the efficacy of the booster on the viral component of Covid wanes this effect will dissipate.
Dr. Prasad’s point is clear, the only way to sort out what is actually happening is to conduct a randomised controlled study where subjects are assigned to vaccination and the matched control group receives a placebo.
Pfizer has the money to do this. So why aren’t they? Possibly because a randomised controlled trial may uncover some potentially serious issues for Pfizer.
Without a carefully designed randomised controlled study, results are subject to the vagaries and inconsistencies of national data collection policies:
- Is Covid data collection mandatory? (In most countries including NZ it is not).
- How carefully are records kept?
- How are Covid hospitalisations defined (for example are pregnant mothers in hospital to give birth who coincidentally test positive for Covid recorded as a Covid patient)?
- How are Covid deaths recorded? How long after a positive test? Do they record whether they had other health conditions?
Let’s look at New Zealand’s current deaths data which illustrates these points:
The proportion of covid deaths by vax status (dark colours) with Proportion of total population in each vax status (light shades)
Shows all deaths ASSOCIATED with covid: ie from any cause within 28 days of a + test. (Unfortunately, the MoH does not release the vax status of CONFIRMED covid deaths)
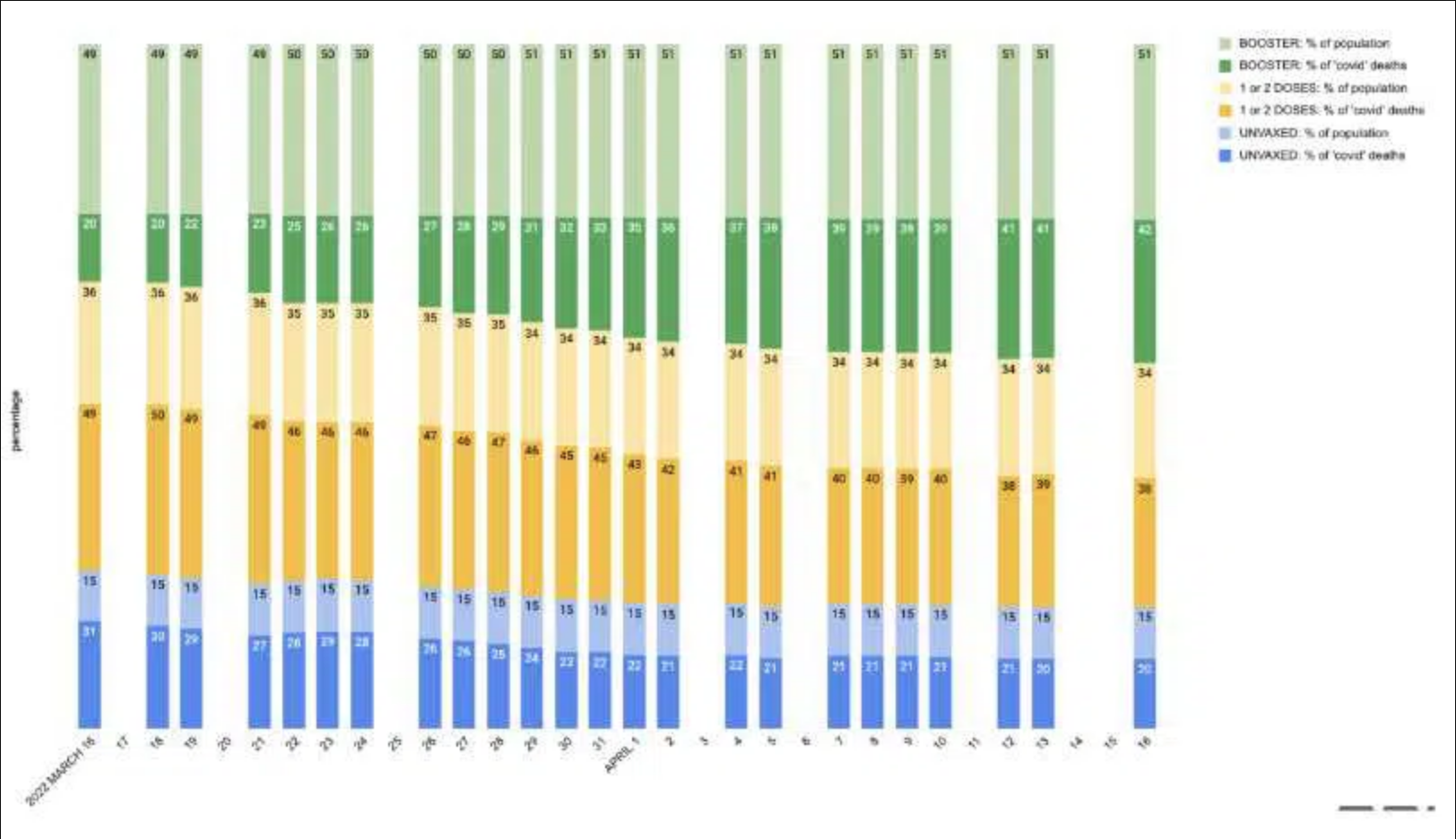
If you read this graph at face value you must conclude as follows:
During the last month boosted individuals have become more vulnerable to death from Covid than they were at the start. Both the vaccinated (excluding the boosted) and unvaccinated groups have become less vulnerable to death through Covid. The increasing vulnerability of the boosted group over time is consistent with the Israeli study. One possible interpretation of the figures is as follows:
The level of natural immunity (due to prior infection) is rising among the unvaccinated as a greater percentage of this group catch and recover from Covid, whereas the more mRNA injections you have appear to inhibit the acquisition of natural immunity.
However few safe scientific conclusions can be drawn from this table.
The New Zealand Ministry of Health does not release sufficient data and the numbers are small. We do not know how many of these deaths were with Covid and how many because of Covid in the various vaccination categories.
We can however segway to figures from the UKHSA. Up until the end of March, the UKHSA conveniently provided the case rates per 100,000 individuals by vaccination status in their vaccine surveillance reports, and the following table has been stitched together by online UK publication The Expose from the case-rate tables found in the Week 3, Week 7 and Week 13 Vaccine Surveillance Reports.
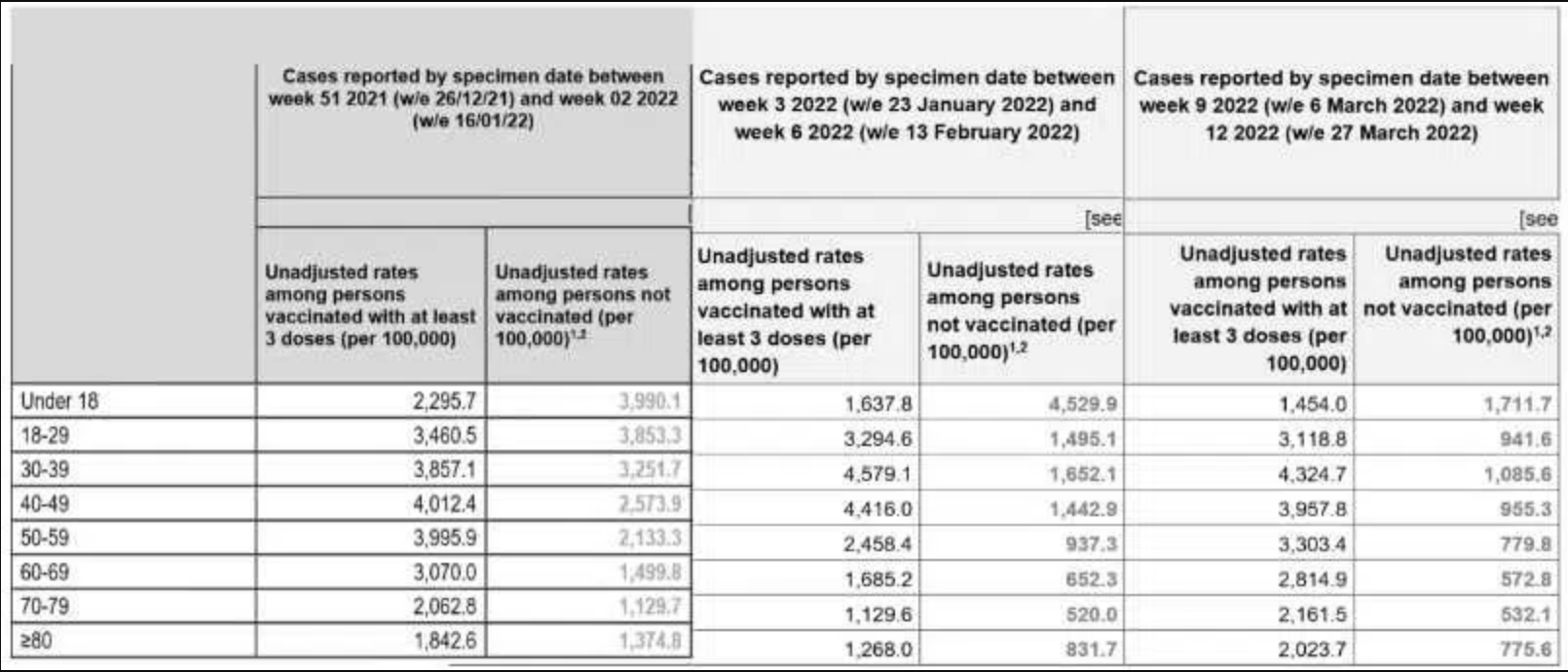
As you can see from the above, the case rates per 100k have been highest among the triple vaccinated population over these 3 months, except for the 18-29-year-olds in the week 3 report only, and the under 18’s in all 3 months.
However, as in New Zealand, the trend is clear: triple vaccinated individuals are becoming more vulnerable and not exhibiting the acquisition of natural immunity in every age category.
A sufficiently well planned and executed randomised controlled trial with a long duration would reveal what is going on, but neither Pfizer or government health agencies are moving in this direction.
In fact, health agencies like the UKHSA are publishing less and less data, possibly because the data is suggesting alarming longer-term health consequences of mRNA vaccination.
The lack of complete data at this point actually confounds the issue because it becomes increasingly difficult to sort out what adverse health effects of Covid are due to infection and which to vaccination. If the supposition that the spike protein is a toxin is right, both will have similar effects to varying degrees.
The action point is clear: mRNA vaccination is not working and could be dangerous. In the absence of reliable clinical assessment, and in the presence of concerning data, the use of mRNA vaccines should be paused.
This article is available to download: Where Did the ‘science’ of the Pandemic Go Wrong and How to Put It Right? (PDF)





{kind=link}