
Table of Contents
BACKGROUND

Puberty blockers are used as part of the process to direct young people who are gender confused towards starting the process of trying to change their sex.
Activists try to argue that they give the child time to figure out if they definitely want to try and change their sex. Here’s the key thing to understand. They don’t pause. They predict. The overwhelming number of children on puberty blockers will go on to wrong sex (cross-sex) hormones.
Puberty blockers are used to delay the changes of puberty and, when taken regularly, they stop the body from making sex hormones. That includes testosterone for boys and oestrogen for girls. So for boys, they slow the growth of facial and body hair, prevent voice deepening, and limit the growth of the penis, scrotum and testicles. For girls this treatment limits or stops breast development and stops menstruation.
Sounds problematic, doesn’t it. Whenever you interfere with the natural process, and especially puberty, there’s always going to be negative consequences.
Puberty blockers, primarily gonadotropin-releasing hormone (GnRH) analogues, are widely promoted as a reversible intervention for children experiencing gender dysphoria. However, emerging evidence challenges the safety, reversibility, and long-term outcomes of these drugs.
<< For a more medical analysis of puberty blockers, please read the submission of Australian paediatrician Dr John Whitehall (author of our report “Children Transitioning: Childhood gender dysphoria – A paediatrician’s warning to New Zealand”) at the bottom of this page >>
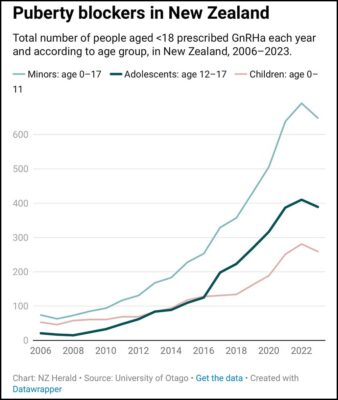
NZ has been prescribing puberty blockers – and at a rate 10x higher per head of population than the UK where puberty blockers have just been banned because of what’s known as the four-year long CASS Review, which concluded that:
- Puberty blockers should no longer be prescribed to children except in the context of research due to these powerful drugs’ effects on brain development and bone health
The CASS report also destroyed the ‘suicide trope’ – better a live son than a dead daughter (or vice versa) – which is used to emotionally manipulate parents into agreeing with their child’s desires, despite the parents’ better judgement and natural concern. The CASS Review said:
- Young people facing gender-related distress had no significantly different levels of suicide risk to other young people with similar levels of complex presentations.
- No evidence that gender-affirming treatment reduces suicide risk.
Here’s what the liberal New York Times reported:
Dr Hilary Cass, a paediatrician who this year published an extensive review of youth gender services in England, said that the delays from the American and British research groups had led the public to believe that puberty blockers improved mental health, even though scant evidence backed up that conclusion… Her report found weak evidence for puberty blockers and noted some risks, including lags in bone growth and fertility loss in some patients.
This is confirmed by other credible research.
A recent Finnish study found that the suicide risk in a large group of adolescents was predicted by the psychiatric problems that often accompany gender distress, not by the gender distress itself.
The Finnish study said:
Although the rate of suicide [in the Finnish study] is just over four times higher among trans young people than their peers, this is explained by their more serious psychiatric problems. When these psychiatric problems are taken into account, there is no evidence that transgender people have a higher rate of suicide.
This Finnish study vindicates their decision four years ago to adopt a more cautious treatment policy which first targets psychiatric, social and educational problems among gender-distressed youth before any assumption of a stable trans identity justifying “experimental” affirmation with hormones or surgery.
The researchers say in their BMJ Mental Health paper:
It is of utmost importance to identify and appropriately treat mental disorders in adolescents experiencing gender dysphoria to prevent suicide; in addition, health policies need to ensure that accurate information is provided to professionals along these lines.
And they studied more than 2,000 gender-referred teens between 1996 and 2019 – 23 years – AND a control group (which many of the pro-trans studies don’t have.)
In other words, the main predictor of mortality in this population is psychiatric morbidity, and medical gender reassignment does not have an impact on suicide risk. That’s the words of the researchers.
A landmark study from the Netherlands (who of course started the Dutch Protocol of doing the steps of transitioning – puberty blockers, cross sex hormones, surgery) published in May 2024 (and conveniently ignored by the media) found that the majority of gender-confused children grow out of that feeling by the time they are fully grown adults.
Researchers in the Netherlands from the University of Groningen tracked more than 2,700 children from age 11 to their mid-20s, asking them every three years of feelings about their gender. Results showed at the start of the research, around one-in-10 children (11 per cent) expressed ‘gender non-contentedness’ to varying degrees.
But by age 25, just one-in-25 (four per cent) said they ‘often’ or ‘sometimes’ were discontent with their gender.
The researchers concluded:
The results of the current study might help adolescents to realize that it is normal to have some doubts about one’s identity and one’s gender identity during this age period and that this is also relatively common.
Studies show up to 93 per cent of children who begin on puberty blockers will go on to receive cross-sex hormone injections. So puberty blockers don’t pause – they predict, and that’s contrary to what you’ll hear trans activists say.
One of the few rigorous studies, which was completed in Sweden, followed a transgender group of adults from 1973-2003. This study found:
Persons with transsexualism, after sex reassignment, have considerably higher risks for mortality, suicidal behaviour, and psychiatric morbidity than the general population. Our findings suggest that sex reassignment, although alleviating gender dysphoria, may not suffice as treatment for transsexualism, and should inspire improved psychiatric and somatic care [restore the natural balance within the body-mind system to resolve physical and mental stress) after sex reassignment for this patient group.
A recent long-term study from Germany also found that a large majority of those diagnosed with gender identity disorders had other mental health conditions. In 2022, 72.4 per cent of individuals with a gender identity disorder diagnosis had at least one other psychiatric diagnosis. The most common co-occurring mental health issues included depressive disorders (affecting about 57.5 per cent of females and 49.3 per cent of males), anxiety disorders (34 per cent of females and 23.5 per cent of males), and borderline personality disorders (17.6 per cent of females and 12.1 per cent of males). Other frequent conditions were attention deficit/hyperactivity disorder (ADHD) and post-traumatic stress disorder (PTSD).
“FAMILY NOISE”

Canadian Kenneth Zucker, one of the leading researchers and clinicians in the world on this topic, and the chair of the group that determined how this issue would be handled in the DSM-5 found that gender dysphoric behaviour and identity in children cannot be addressed without looking at what he calls “family noise”. Gender dysphoria seldom manifests in a child isolated from other factors, particularly those existing within the family dynamic. This is strongly verified when observing the family interactions of such children as well as their parents’ reaction to these children. So it’s often driven by the convictions of the parents rather than the child.
The Amsterdam Gender Identity Clinic, one of the largest clinics in Europe treating gender dysphoric children, looks at a host of larger satellite issues with the child and their family beyond the dysphoria itself. These would include parallel emotional, behavioural and family issues that might be present that could impact the child’s dysphoria. They explain dysphoria does not generally stand alone.
As we have always said, we should heal the mind, not cut the body.
A WORLDWIDE TREND…
- France 2024: French senators have published a report that expresses alarm at the excesses of child gender transition and have proposed a bill to put an end to it.
- England 2024: The United Kingdom [has] indefinitely banned new prescriptions of puberty blockers to treat minors for gender dysphoria. The indefinite ban on the medication in Britain comes several months after an independent study commissioned by England’s National Health Service concluded that the medical evidence around transition-related care for minors is “remarkably weak” and that more research is needed. “Children’s healthcare must always be evidence-led,” British Health and Social Care Secretary Wes Streeting said in a press release. “The independent expert Commission on Human Medicines found that the current prescribing and care pathway for gender dysphoria and incongruence presents an unacceptable safety risk for children and young people.”
- The Netherlands 2024: The Dutch government has passed a motion to conduct research into the physical and mental health outcomes of children given puberty blockers.
- Denmark 2023: In a marked shift in the country’s approach to caring for youth with gender dysphoria, most youth who are referred to the centralised gender clinic now receive therapeutic counselling and support, rather than a prescription for puberty blockers.
- Germany 2024: The 2024 German Medical Assembly, a convention with delegates from 17 medical societies, passed a resolution to restrict medical interventions on gender-questioning minors to research settings. Votes were overwhelmingly in favour (120 for, 47 against, and 13 abstentions).
- Norway 2023: After a review, the Norwegian Healthcare Investigation Board stated it has serious concerns about the treatment of gender dysphoria in children and that the current ‘gender affirming’ guidelines are not evidence-based and must be revised.
- Italy 2024: Initiated a review of puberty blockers.
- Sweden 2021: The Karolinska Hospital ceased the use of puberty blockers for those aged under 18.
- Finland 2020: revised its treatment guidelines, prioritising psychological interventions and support over medical interventions.
- USA 2023–24: A total of 26 states have so far passed laws protecting children from routine medicalisation of gender distress. The laws vary in what they proscribe and in the penalties imposed and some of them are subject to ongoing legal challenges. This interactive map provides state by state details. The US Supreme Court is currently weighing the constitutionality of a Tennessee ban on gender-affirming care for minors. Tennessee is one of more than two dozen states that restrict such care in the US. The Food and Drug Administration (FDA) in the US issued a warning label about the risk of puberty blockers.
- WHO 2024: the World Health Organisation decided not to pursue guidelines for children and adolescents because “the evidence base for children and adolescents is limited and variable regarding the longer-term outcomes of gender affirming care…”
Professor Christopher Gillberg, an expert in child and adolescent psychiatry, and who gave expert evidence in the British High Court regarding Keira Bell’s harmful transitioning believes prescribing drugs to delay puberty is a scandal and tantamount to conducting ‘a live experiment’ on vulnerable children. He said:
In my years as a physician, I cannot remember an issue of greater significance for the practice of medicine. We have left established evidence-based clinical practice and are using powerful life-altering medication for a vulnerable group of adolescents and children based upon a belief.
THE MINISTRY WRONGLY RELIES ON WPATH (& PATHA)
WPATH stands for the World Professional Association for Transgender Health. WPATH guidelines are considered the gold standard for the field of health care for those diagnosed with gender dysphoria, and are widely used in hospitals and clinics across the US, Canada, and the UK and are highly influential to some major medical groups.
The Society for Evidence Based Gender Medicine (SEGM), an international group of more than 100 clinicians and researchers, responded to ‘the science’” and wrote a critique , citing the potential for harm due to WPATH’s lack of methodological rigor and very low-quality evidence. WPATH says its guidelines were written “based on available evidence” but cite flawed, cherry-picked studies to support their conclusions. “The current description of the literature betrays a strong bias toward studies promoting social and medical transition,” said SEGM.
Carl Heneghan, editor-in-chief of the British Medical Journal, and Professor of Evidence-Based Medicine from the University of Oxford performed a review of the literature for puberty blockers and cross-sex hormones in children and adolescence. He concluded: “The current evidence base does not support informed decision making and safe practice in children.”
Thousands of doctors worldwide rely on WPATH including our own Ministry of Health Te Whatu Ora – and it’s pushed by the radical association of NZ activists called PATHA (Professional Association for Transgender Health Aotearoa).
Transgender research and policy comes out of the University of Waikato’s Trans Health Research Lab. Unfortunately, the unit is driven by activists and an agenda, rather than science and independent research. The director is a trans woman who just also happens to be on the executive committee of WPATH. Another associate investigator is Green MP Elizabeth Kerekere – say no more!
We’ve written in detail on the weakness and flaws of the Counting Ourselves survey that the unit does:
https://freetolive.nz/2021/10/22/counting-ourselves-advocacy-research-should-be-treated-with-caution/
MINISTRY HAVE PREVIOUSLY HAD TO BACK DOWN
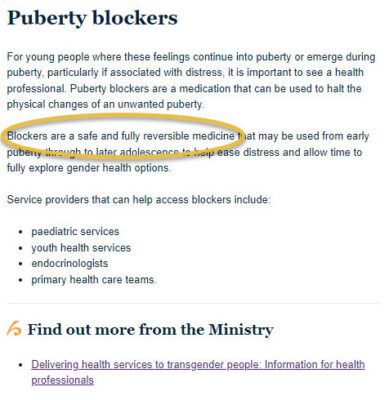
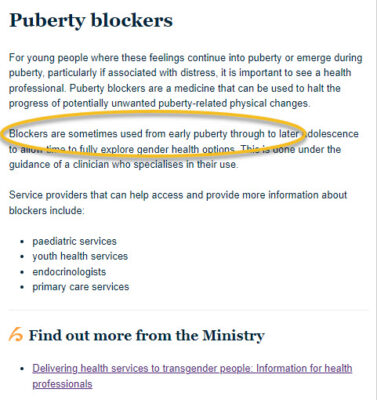
The Ministry of Health previously proclaimed that puberty blockers are “safe and fully reversible”. But overnight – and without announcement – it was subtly changed.
Medical professionals and medical groups – including The Royal Australian and New Zealand College of Psychiatrists (RANZCP) – recently sounded growing international concern around the use of puberty blockers to treat young people with gender dysphoria because of the low certainty of benefits but the significant potential for medical harm.
BEFORE 16 SEP 2022 AFTER 16 SEP 2022
WHAT DID THIS LATEST MINISTRY OF HEALTH REVIEW FIND?
The Evidence Review found a lack of good quality evidence for the effectiveness or safety of puberty blocking treatment in young people with gender dysphoria. We do not have good evidence to say that the medicines used improve the longer-term outcomes for young people with gender-related health needs – nor that the potential longer-term risks are low.
Wow – that is damning. That should be the end of it. When would you prescribe something that lacks good quality evidence, and has no evidence that improves outcomes or how bad the risks are? You wouldn’t.
And any parent who has a doctor who wants to prescribe them for their child should be shouting – hell no!
CONCLUSION
There is insufficient quality evidence to ensure that clinicians advising on puberty blockers can meet their professional practice and ethical standards such that their patients can give properly informed consent to the use of puberty blockers.
Consent for under 16-year-olds is not possible. In New Zealand, consent to medical treatment can be given by legal minors of or over the age of 16 years as set out in section 36 of the Care of Children Act 2004. Under common law, Gillick competence is used to establish if an adolescent under 16 years is capable of giving consent to medical treatment. Gillick competence is about determining when a person under 16 can consent to their own medical treatment without the need for parental permission or knowledge. Lord Scarman’s test is generally considered to be the test of ‘Gillick competency’. He required that a child could consent if they fully understood the medical treatment that is proposed:
As a matter of law the parental right to determine whether or not their minor child below the age of 16 will have medical treatment terminates if and when the child achieves sufficient understanding and intelligence to understand fully what is proposed.
But consent is not possible when there is insufficient evidence about the efficacy of the treatment or the resultant complications following use of puberty blockers; put another way, it is impossible for anyone – let alone an under 16 – to consent to a treatment that itself is not understood nor has sufficient evidence to support it.
WATCH THE TESTIMONY OF CHLOE COLE
NOW WE NEED YOU
The Ministry of Health still needs further persuading, surprisingly. The ministry is considering whether further measures need to be put in place to ensure no children or young people are unduly exposed to unknown risks.
READ the letter we have just sent to the Director-General of Health with legal advice that says that prescribing puberty blockers could be illegal
READ our submission to the Ministry of Health.
READ our Fact Sheet above which summarises some of the recent research on puberty blockers.
And then COMPLETE THE CONSULTATION ONLINE
or
EMAIL pbconsultation@health.govt.nz to share your thoughts.
HERE’S THE QUESTIONS THEY WANT YOU TO ANSWER
(If emailing, just answer these question)
Question 1: What is your main interest in the consultation topic?
Question 2: Do you live in New Zealand?
Question 3: Publishing submission (can be done anonymously)
Question 4: Official information Act responses (your submission is open to the public, but you can request all identifying information is NOT made available)
KEY QUESTIONS
Question 5: In your view, how should puberty blockers be prescribed for gender-affirming care in New Zealand?
They shouldn’t. “Gender affirming care” is a contradiction.
Question 6: Who do you think should be able to start patients on treatment with puberty blockers?
They shouldn’t. They are not effective or safe – as the Ministry of Health has already established and is the reason more and more countries are banning their use.
Question 7: Which young people should be able to receive treatment with puberty blockers for gender dysphoria?
They shouldn’t. They are not effective or safe – as the Ministry of Health has already established and is the reason more and more countries are banning their use.
Question 8: If prescribing of puberty blockers is restricted by regulation, how might this affect you and/or the people that you represent?
It would enable confused vulnerable young people to get the counselling support they need to live comfortably in their biological body while expressing their own personality and traits.
Question 9: Do you have any further views on how any regulation should be designed?
They should be immediately banned for children with any form of gender dysphoria.
SUBMISSIONS CLOSE MONDAY, 20 JANUARY 2025 5:00PM.
They’re hoping you’ll forget. Disappoint them!
Why not do it before Christmas – as a gift to vulnerable young people who just need counselling and affirmation – not chemicalisation and castration.
MEDICAL DETAIL
Summary from Professor John Whitehall
Foundation Chair and Professor of Paediatrics and Child Health at the University of Western Sydney.
Introduction
Puberty blockers, primarily gonadotropin-releasing hormone (GnRH) analogues, are widely promoted as a reversible intervention for children experiencing gender dysphoria. However, emerging evidence challenges the safety, reversibility, and long-term outcomes of these drugs. The following submission outlines scientific, medical, and ethical concerns regarding the administration of puberty blockers to children.
- Lack of Scientific Consensus and Evidence-Based Practice
The use of puberty blockers for gender dysphoria is currently lacking robust, long-term studies to validate their safety and efficacy. This is a significant departure from established protocols, as these drugs were initially developed to treat conditions like precocious puberty. The absence of comprehensive research on the long-term effects of puberty blockers, particularly concerning cognitive, neurological, and psychological development, is a cause for concern.
- Absence of Long-Term Data:
- There is an absence of comprehensive research on the long-term effects of puberty blockers, particularly regarding cognitive, neurological, and psychological development. For instance, studies on mice and humans indicate that blocking GnRH disrupts brain development and executive functioning, with potential impacts on memory, cognition, and emotional regulation[i][ii].
- The irreversible nature of certain side effects—such as infertility and impaired sexual function opposes claims of full reversibility.
- While advocates argue that puberty blockers “buy time” for children to explore their gender identity, there is a lack of substantive evidence demonstrating improved outcomes in mental health or life satisfaction post-treatment. On the contrary, many individuals, such as detransitioners, report regret or unanticipated negative consequences of undertaking puberty blockers.
- Experimental Nature:
- Critics of puberty blockers, including leading medical experts, argue that their use constitutes experimentation. WPATH members themselves have acknowledged the lack of rigorous studies on outcomes such as fertility and the ability to achieve orgasm post-treatment[iii].
- The Dutch protocol, often cited as a foundational study supporting the use of puberty blockers, has faced criticism for its methodological weaknesses, including small sample sizes, lack of control groups, and short follow-up periods[iv]. This raises significant concerns about the reliability of its conclusions.
- Global Shifts in Practice:
- Countries such as Sweden, Finland, and the UK have begun to roll back or limit the use of puberty blockers in response to mounting evidence of harm and the lack of demonstrated long-term benefits. For instance, the closure of the Tavistock Clinic in the UK followed an independent review highlighting systemic deficiencies in the evidence supporting these treatments[v].
- Adverse Effects on Neurological and Cognitive Development
GnRH plays a critical role in brain development beyond its reproductive functions. Blocking this hormone interrupts processes essential for neuronal growth, connectivity, and maintenance.
- Neurological Consequences:
- Research reveals that puberty blockers can lead to hypertrophy and dysregulation in brain regions like the limbic system, which integrates cognition, memory, and emotions.
- Human MRI studies have documented the impacts of undergoing GnRH blockade in adolescents. One study found in an adolescent natal boy administered ‘blockers’ (to pursue a female identity) that expected structural development of the brain did not occur and was associated with a reduction in IQ[vi]. In another MRI study of otherwise healthy women, it was found blockers interfered with neuronal connectivity in the limbic region and were associated with the ‘emergence of depressive symptoms[vii].
- The effect of puberty blockers on the limbic system should not be under-estimated. Especially considering that part of the brain coordinates cognition, emotion, memory and desire into ‘executive function’. It is biologically implausible, therefore, to proclaim that ‘blocking’ puberty permits time for mature consideration of gender and the mechanism and results of its hormonal and surgical re-orientation to a gender incongruent with chromosomes.
- Kallmann Syndrome (KS) is a rare condition with significant abnormalities in the brain, revealed through MRI scans. For various genetic reasons, GnRH cells and olfactory cells, which originate together in the nasal region of the embryo, fail to migrate properly into the brain[viii]. This results in two major issues: a diminished sense of smell and failure to undergo puberty due to the lack of GnRH production.
- Apart from these, major structural abnormalities in the brain have been noted. Research by Manara et al. suggests profound structural changes in the basal forebrain in KS patients, far beyond the simple hypoplasia of the olfactory sulcus.[ix] Given the consistency of these brain abnormalities, it is likely due to the absence of GnRH. Despite the need for more studies, the existing evidence should caution against the unqualified assertion that puberty blockers are entirely safe and reversible.
- Cognitive and Behavioural Impacts:
- In research with animal models, puberty blockers were associated with increased emotional lability, preference for familiar over novel environments, and impaired decision-making.[x] Such effects raise concerns about children’s ability to provide informed consent for life-altering treatments.
- Furthermore, GnRH plays a neuro-modulatory role, crucial for the development and maintenance of brain connectivity. Blocking its function can disrupt processes critical for cognitive development, as evidenced by studies showing reduced neuronal connectivity and executive function impairments in BOTH animals and humans[xi][xii].
- Effects on the adolescent brain
- The adolescent brain undergoes significant reorganisation during puberty, driven in part by the hormonal surges initiated by GnRH. These changes are essential for the maturation of executive functions, emotional regulation, and social cognition.
- Puberty blockers interrupt this natural process, potentially leading to long-term deficits in these areas. For instance, MRI studies have shown that adolescents on GnRH analogues exhibit arrested brain development compared to their peers, with reduced growth in areas critical for higher-order thinking and emotional control.[xiii] Additionally, by halting the natural hormonal processes, puberty blockers may exacerbate pre-existing mental health challenges, such as anxiety and depression, which are prevalent among gender-diverse youth.
- Ethical Concerns and Informed Consent
Puberty blockers are often prescribed to children with coexisting mental health challenges, yet their ability to comprehend the implications of such treatments remains questionable.
- Inadequate Understanding Among Patients and Parents:
- Leaked files from The World Professional Association for Transgender Health (WPATH) discussions exchanged, from 2021 to 2023, between WPATH members and leaders on an ‘internal on-line forum for discussing specific medical cases’, and during an ‘Identity Evolution Workshop’ on May 6, 2022 reveal that even well-educated parents struggle to grasp the complexities of these interventions fully. Children, often as young as nine, are less equipped to understand risks, including irreversible infertility and altered brain development[xiv][xv].
- Notably, the leaked WPATH files highlight professionals’ own doubts about patients’ comprehension. One expert from the files, an endocrinologist Dan Metzger warned ‘the thing you have to remember about kids is that we’re often explaining these sorts of things to people who haven’t even had biology in high school’. One contributor to WPATH guidelines admitted that explaining the long-term consequences of puberty blockers like sterilisation and infertility to young patients is akin to “talking to a brick wall,” underscoring the inadequacy of informed consent.
- Autonomy vs. Protection:
- Disregarding the question of whether any child possesses sufficient maturity of cognitive power to digest and responsibly act on such complicated, life-changing matters, even if cognition is not limited by drugs, it should not be forgotten the brains of almost all gender-confused children are also burdened by associated neurodevelopmental challenges such as autism, and lasting traumas of social disruption [xvi].
- While proponents of gender-affirming care emphasise respecting the autonomy of gender-diverse youth, minors lack the developmental capacity for informed decision-making. The irreversible consequences of puberty blockers contradict ethical principles of beneficence and non-maleficence.
- For example, In Australia, in recognition of the ‘childish brain’, the minimum age of criminal responsibility is held to be 10 years. Between the ages of 10 and 14 years, on the presumption a child is incapable of committing a criminal act, he or she can only be convicted if the prosecution can prove the child can distinguish between right and wrong. From 14 to either 17 or 18 years (depending on jurisdiction), adolescents may be held responsible for criminal acts but are subject to different penalties than adults. Other countries have higher ages for accountability.
- In contrast, in Guidelines from the Royal Children’s Hospital Melbourne, there is no age limit for the administration of so-called ‘affirmation therapy’ of a confused child to a gender incongruent with chromosomes. For example, if a child with male chromosomes believes he is a girl, there are no age limits on social affirmation, the administration of ‘puberty blockers’, or of ‘cross-sex hormones’ in pursuit of similitude with the opposite gender. Though mastectomy is generally reserved for those over 16, Family Court records reveal breasts have been removed from 15-year-old girls.
- The distorted application of “informed consent” transforms the patient-physician relationship into one of consumer-provider, undermining the ethical responsibility of medical professionals to guide decisions based on comprehensive understanding and best interests.
- Escalation to Irreversible Treatments
Puberty blockers frequently act as a gateway to cross-sex hormones and irreversible surgeries.
- High Transition Rates:
- Data indicates that nearly all children who start on puberty blockers progress to cross-sex hormones. This sequential process undermines the narrative that puberty blockers simply provide a “pause” for reflection.
- Physical and Psychological Harms:
- Cross-sex hormones have been linked to significant side effects, including cardiovascular risks and altered brain morphology. Surgical interventions carry a high risk of complications, as demonstrated by reports of pain, infection, and regret among detransitioners.
- Two independent studies based on MRI imaging have revealed the male brain shrinks at a rate multiples faster than in ageing, after only a short period of administration of oestrogen in the process of transgendering. It is presumed brain cells ‘apoptose’ which is a euphemistic term for ‘die’[xvii][xviii]. Receiving testosterone in the process of transgendering, the female brain hypertrophies, that is, swells, for reasons unknown apart from the fact that there is no increase in neurons[xix].
- Reports from the Sydney Children’s Network reveal alarming trends, including minors undergoing double mastectomies, hysterectomies, and complex genital surgeries. Such irreversible procedures underscore the trajectory from puberty blockers to life-altering interventions.
- Contradictory Claims of Reversibility
Proponents of puberty blockers assert their effects are reversible. However, evidence from both clinical settings and leaked discussions among professionals suggests otherwise:
- Impact on Sexual Development:
- The five stages of puberty described by British Physician, James Tanner’ Stage 2 corresponds with development of breast buds in girls and testicular enlargement in boys, around 9 years of age. Stage 4 corresponds, a few years later, with the production of eggs and sperm. Puberty blockers administered at Tanner Stage 2 hinder normal sexual maturation, with reports of individuals losing the ability to achieve orgasm.
- Puberty blockers will not only stop the production of eggs, sperm, oestrogen and testosterone, but also the growth of genitalia and sex specific features such as breasts and beards.
- Infertility:
- Early GnRH blockade halts the development of gametes, leading to irreversible infertility in most cases.
- Alternative Approaches
Instead of medicalising gender dysphoria in children, alternative therapeutic approaches should be explored:
- Psychotherapy:
- Studies show that most gender-diverse children reconcile with their biological sex when supported with non-invasive, traditional therapeutic interventions.
- Addressing Coexisting Disorders:
- Many children presenting with gender dysphoria have underlying psychological conditions, such as autism or depression. Addressing these co-morbidities is essential before considering irreversible interventions like the use of puberty blockers or cross-sex hormones.
Conclusion
The current use of puberty blockers for gender dysphoria lacks sufficient scientific validation and carries significant risks of harm. Given the non-reproductive, neurological role of GnRH has been discussed for decades and is based on studies from many centres throughout the world, is it odd the only people who appear to be, at best, unaware of its implications are practitioners in gender clinics for children who blithely seek to assure, from Tavistock to Melbourne, that ‘blockers are safe and entirely reversible’ and continue to administer them to vulnerable children. Furthermore, there is much more warning about the side effects of puberty blockers than there ever was over the side effects of thalidomide on developing babies.
Therefore, the administration of puberty blockers to children is fraught with risks and uncertainties, with profound implications for their physical, neurological, and psychological health. This submission calls for the suspension of the use of puberty blockers for gender dysphoria. A more cautious, evidence-based, and ethically sound approach that safeguards the well-being of vulnerable children would be the more…
[i] Anacker C et al. Behavioural and neurobiological effects of GNRH agonist treatment in mice-potential implications for puberty suppression in transgender individuals. Neuropsychopharmacology. 2021;46:882-890.
[ii] Pfaff D, Luteinising hormone releasing factor potentiates lordosis behavior in hypophysectomised ovariectomised female rats. Science. 1973. 182:1148-1149.
[iii] Files: 210.
[iv] Ristori J, Steensma TD. Gender dysphoria in childhood. International review of psychiatry. 2016 Jan 2;28(1):13-20.
[v] https://www.newstatesman.com/politics/health/2024/03/inside-the-collapse-of-the-tavistock-centre
[vi] Schneider MA, Spritzer PM, Soll BM et al. Brain maturation, cognition and voice pattern in a gender dysphoria case under pubertal suppression. Front Hum Neurosci. 2017;11:528. Doi:10.3389/fnhum.2017.00528.
[vii] Fisher PM, Larsen CB, Beliveau V. Pharmacologically Induced Sex Hormone Fluctuation Effects on Resting-State Functional Connectivity in a Risk Model for Depression: A Randomized Trial. Neuropsychopharmacology (2017) 42, 446–453
[viii] R. Manara, A. Salvalaggio, A. Favaro et al. Brain Changes in Kallmann Syndrome. Am J Neuroradiol 35:1700 – 06 Sep 2014. http://dx.doi.org/10.3174/ajnr.A3946
[ix] R. Manara, A. Salvalaggio, A. Favaro et al. Brain Changes in Kallmann Syndrome. Am J Neuroradiol 35:1700 – 06 Sep 2014. http://dx.doi.org/10.3174/ajnr.A3946
[x] Robinson, J. E., Evans, N. P., Dumbell, R., Solbakk, A. K., Ropstad, E., and Haraldsen, I. R. (2014). Effects of inhibition of gonadotropin releasing hormone secretion on the response to novel objects in young male and female sheep. Psychoneuroendocrinology 40, 130–139. doi: 10.1016/j.psyneuen.2013. 11.005
[xi] Hough D, Bellingham M, Haraldsen I et al., 2017 Spatial memory is impaired by peripubertal GnRH agonist treatment and testosterone replacement in sheep. Psychoneuroendocrinology. 2017; 75:173-182.
[xii] Prange-Kiel J, Jarry H, Schoen M et al. Gonadotrophin releasing hormone regulates spine density via its regulatory role in hippocampal oestrogen synthesis. J Cell Biol. 2008;180:417-426.
[xiv] Files: 210.
[xv] Block J. Dispute arises over World Professional Association for Transgender Health’s involvement in WHO’s trans health guideline. bmj. 2024 Oct 30;387.
[xvi] Mull D, Versluis-den Bieman HJ, Slijper FM et al. Phychological assessments before and after treatment of early puberty in adopted children. Acta Paediatr. 2001;90(9):965-971.
[xvii] Hulshoff Pol HE, Cohen-Kettenis PT, Van Haren NE, et al. Changing your sex changes your brain: Influences of testosterone and estrogen on adult human brain structure. Eur J Endocrinol. 2006;155(1):S107–S111. Doi 10.1530/eje.1.02248
[xviii] Zubiaurre-Elorza, L., Junque, C., Gomez-Gil, E., & Guillamon, A. (2014). Effects of cross-sex hormone treatment on cortical thickness in transsexual individuals. Journal of Sexual Medicine, 11, 1248–1261.
[xix] Guillamon A, Junque C, Gomez-Gil E. A Review of the Status of Brain Structure Research in Transsexualism. Arch Sex Behav 2016 Oct; 45(7):1615–1648.
This article was originally published by Family First New Zealand.







