
Table of Contents
NZDSOS
NZ Doctors Speaking Out with Science
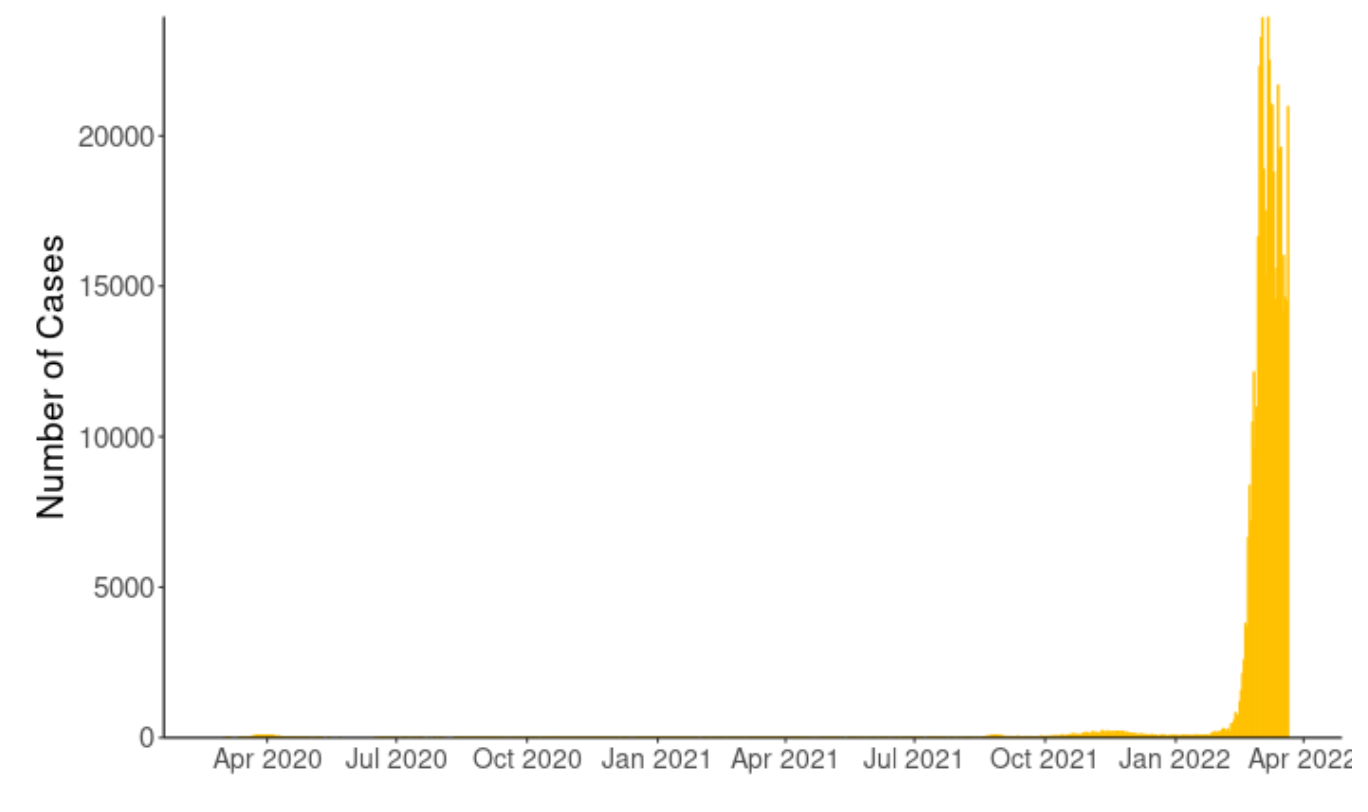
We are currently at the peak of the biggest outbreak of COVID-19 since the pandemic began two years ago. As can be seen by the Ministry of Health image below. Over the weekend, mainstream media reported New Zealand’s deadliest day with twenty people having died with Covid.
The meaningless with- and not of- Covid statement aside, based on an Official Information Act request (OIA), New Zealand Doctors Speaking Out with Science (NZDSOS) is questioning the accuracy of the numbers of Covid-19 cases and thus deaths.
In Wednesday’s press conference Prime Minister Ardern mentioned in passing, that the number of cases is more likely to be over one million. We assume this is based on a combination of test results from PCR and Rapid Antigen Tests (RATs) and undefined modelling.
1. Cases in New Zealand
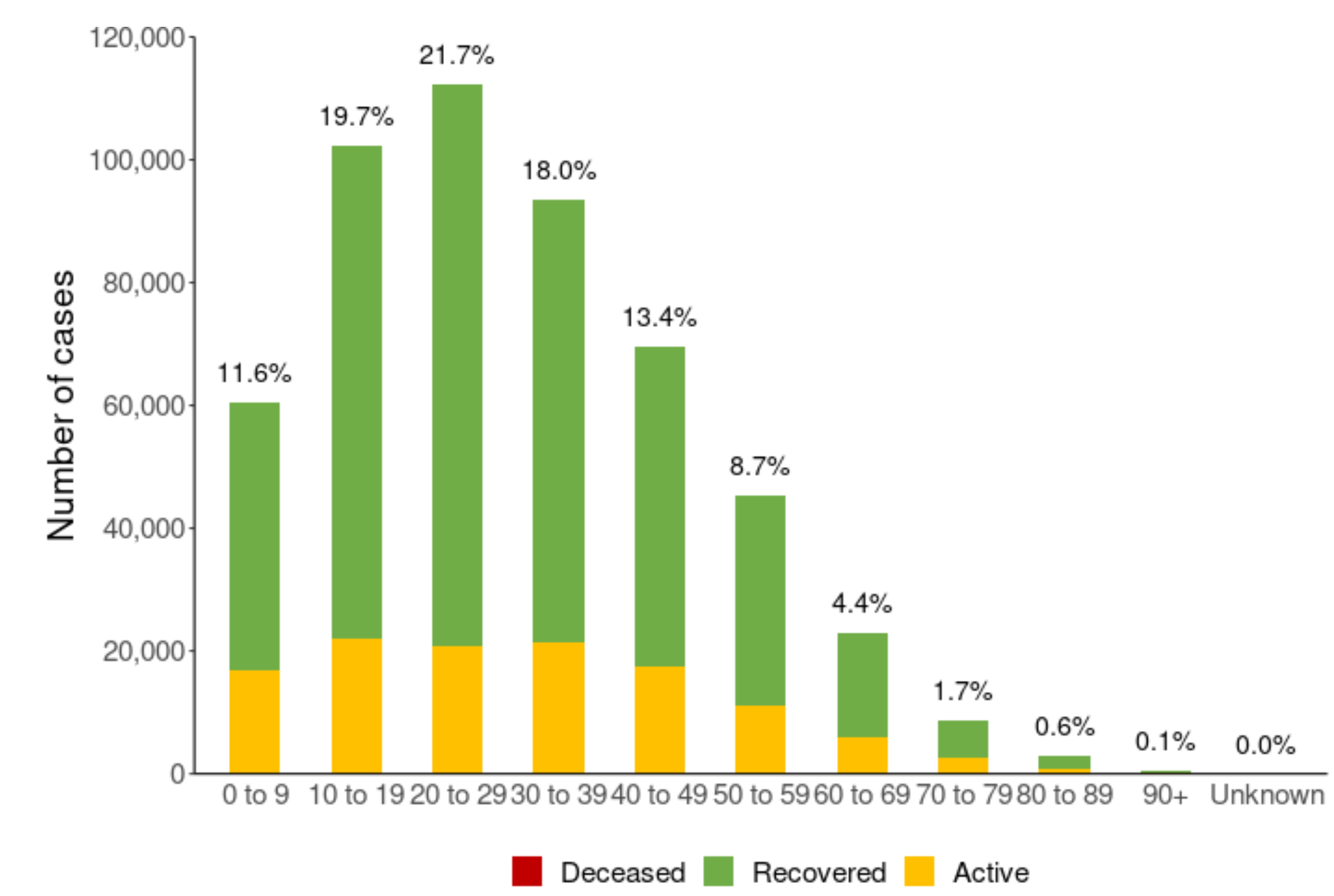
The Ministry of Health (MoH) is currently recording about 20 000 new “cases” (purely based on reported test results) of COVID-19 daily. A quick look at the ministry’s website indicates almost all of New Zealand’s cases have occurred since February. Most of the cases seem to be in the under 40 year age group.
2. Validity of Polymerase Chain Reaction (PCR) and Rapid Antigen (RAT) tests.
Most of the recent test results are likely to be RATs results. RATs compare favourably to PCR in those who are symptomatic, including for the detection of Omicron. The MoH indicates RATs are most accurate in those who have symptoms. However, RATs have been widely used for travel, employment and by individuals who have been in contact with a “positive case” but are otherwise well.
The MoH advises a PCR test is “highly accurate” under ideal conditions (these are not specified) and stresses that in real life there is a risk of a false negative results. It downplays possible false positives results.
NZDSOS are in receipt of an Official Information Act response the MoH referred to ESR in regard to PCR accuracy.
The question asked to the MOH was:
‘Please disclose all MoH testing protocol documentation benchmarks, test parameters and uniquely evidential virus markers used by the NZ Testing Laboratories to prove and verify the presence of Live SARS Cov-2 virus and no other viral presence from the sample?’
The answer given was:
The Polymerase Chain Reaction (PCR) and other molecular tests which they [diagnostic laboratories] perform are specific in detecting parts of SARS-CoV-2 RNA. The presence of the virus’ RNA does not necessarily mean that it came from infectious virions as it could also be from broken up viral components and therefore a PCR, or other molecular tests, cannot verify the presence of live virus SARS-CoV-2. The molecular tests are specific to detect SARS-CoV-2 which means one cannot exclude the possibility that other pathogens, like other viruses, are not also present. In most cases, no additional diagnostic tests are performed to exclude co-infection (emphasis added).
It would appear, a positive PCR test tells us certain sequences of RNA were found in the sample. However, it cannot tell us if these RNA sequences indicate the presence of live SARS-CoV-2 (the virus that supposedly causes COVID-19) alone, nor more importantly, whether the person from whom the sample has been taken is infectious. Even if the person had symptoms and SARS-CoV-2 RNA was detected, it is absolutely possible the symptoms were caused by a different ‘germ’ altogether as other ones weren’t excluded.
The MoH states “we expect very few (if any) false-positive test results with PCR.” We would like to refer the MoH to the facts from their Research Institute.
Instead of considering these facts, it appears the Ardern government has inflicted significant harm to New Zealand on the basis of positive tests, which are nothing more than non-verified RNA sequences of dubious significance.
3. Case classification
A long-standing rubric in medicine is that a diagnosis (case) is made on a combination of history, clinical symptoms and possibly laboratory testing. The latter is actively discouraged. Even in flu season, only a certain number of ‘index’ general practices undertake flu testing in symptomatic patients. If a GP who is not in one of the ‘index practices’ requests a flu test, they are likely to get an unfriendly call from their local microbiologist wanting justification for requesting this unnecessary test.
Therefore, flu cases are counted as positive tests in those with symptoms.
With regard to COVID “cases”, the MoH can determine that a person who has had SARS-CoV-2 detected from a clinical specimen is not a case if they have undergone further investigations such as serology (blood tests), repeat testing, history, and symptoms which are negative.
We are not aware of one single negative case where the individual has been contacted by the MoH to determine whether they could be a false positive.
As the RATs compare with PCRs, it is possible that RAT testing suffers from the same flaws as the PCR. While we cannot be sure of this, we would expect the Ministry of Health and the Prime Minister to consider the limitations of the data that they are using to impose restrictions on New Zealanders.
Given that many asymptomatic people are using a flawed test, NZDSOS questions the validity of positive test numbers. Furthermore, as a positive test may be false and few – if any – individuals are being followed up, we suggest positive tests do not necessarily indicate cases of COVID-19.
Given the age distribution of positive tests, are individuals under 40 vulnerable to positive tests rather than to COVID-19?
Why is the Ardern government, MoH and its media continuing to scare the New Zealand public with positive test numbers? Is the motivation political rather than for public health?





{kind=link}